954-792-4663
 PSA Screening for Prostate Cancer, the Failed Medical Experiment
PSA Screening for Prostate Cancer, the Failed Medical Experiment by Jeffrey Dach MD
Jim Smith is a 55 year old athlete and outdoors man, who runs marathons and camps out. He was not at all worried about prostate cancer until he saw the Larry King Live Show endorsing PSA screening for prostate cancer. Larry King played clips showing celebrity endorsements from Colin Powell, Joe Torre, Don Imus, Charlton Heston, Jerry Lewis, Arnold Palmer, Rudy Giuliani, John Kerry, Bob Dole, Norman Schwarzkoff, John McEnroe and Michael Milken all relating personal prostate cancer stories. Watching all these celebrities urging PSA testing on the Larry King show lured Jim into a local Miami hospital offering free screening for prostate cancer.
Above left image: Larry King courtesy of wikimedia commons.
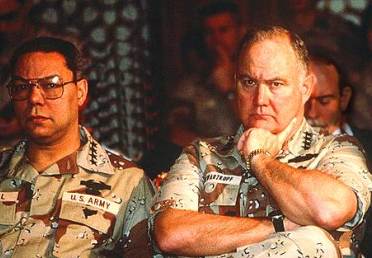 Above image: Colin Powell and Norman Schwarzkopf at Press Conference Desert Storm 1991. Same expression frequently seen on men contemplating prostate biopsy. Images courtesy of wikimedia commons.
Above image: Colin Powell and Norman Schwarzkopf at Press Conference Desert Storm 1991. Same expression frequently seen on men contemplating prostate biopsy. Images courtesy of wikimedia commons.
Jim’s PSA test showed an elevated PSA of 4.7 (normal is less than 4), so Jim was sent over to a local urologist office all set for a needle biopsy of his prostate.
Working as an interventional radiologist for many years, I actually pioneered ultrasound guided prostate biopsies, and taught many urologists how to do the procedure. This procedure involves placing an ultrasound probe into the patient’s rectum to image the prostate, and advance a long needle into the prostate gland for the tissue sample. (repeated a number of times). As uncomfortable as it sounds, it’s really all not that bad.
Thinking the rush to biopsy was a bit hasty, Jim declined, and instead came to my office seeking a second opinion. After a brief chat, Jim complained of recent urinary symptoms. Sure enough, his lab findings indicated a simple infection of the prostate gland which is quite common.

Left Image: Bob Dole smiling ear-to-ear courtesy of Wikimedia Commons.
Inflammation and prostate infection is a common cause of PSA elevation. The plan was to treat Jim with antibiotics for his prostate infection and repeat the PSA test. After a few weeks of daily Ciprofloxin, Jim was smiling ear-to-ear because his repeat PSA was back down to 3.8 and his doctors no longer advised prostate biopsy.
PSA is Prostate Specific Antigen, a protein discovered in 1986, and a marker for prostate cancer and inflammation. This article will show you that PSA screening for prostate cancer is, in fact, a 20 year failed medical experiment which provides little or no benefit in saving lives.
Gina Kolata of the New York Times wrote a scathing indictment of PSA screening citing two studies published from March 2009 New England Journal of Medicine, considered the most important studies in the history of men’s health.
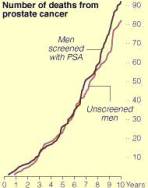
The large US study, the PLCO, showed no mortality benefit from PSA screening. (see left chart). The Europeans, on the other hand, did much better. Their ERSPC study provided a 20% mortality reduction from PSA screening. However, this came at a high cost of significant over-diagnosis. Fifty men were treated for prostate cancer unnecessarily for every life saved. This treatment of surgery, radiation and hormonal castration is associated with erectile dysfunction (ED) and incontinence.
Left Chart: Courtesy of NEJM PLCO study data, Gina Kolata, NY Times. Note Men screened with PSA (black line) has higher mortality then unscreened men (red line).
Welch reported a very unpleasant finding in the August 2009 issue of the Journal of the National Cancer Institute. Since the invention of the PSA test in 1986, one million men have been treated for a clinically insignificant prostate cancer that did not require treatment. These are 1 million male victims, many suffering from side effects of treatment, such as erectile dysfunction and incontinence.
 Left Image: Million Man March courtesy of Wikimedia Commons.
Left Image: Million Man March courtesy of Wikimedia Commons.
Take a look at the charts Welch used to arrive at his conclusions.
See charts below: The upper brown data line shows annual incidence rate of prostate cancer, (the incidence). The lower chart shows mortality which was stable at 30,000 deaths per year. Notice the huge spike in detected cases when PSA testing was introduced (red arrow). Notice the INCREASE in Mortality in the lower chart (blue arrow) the same years as a spike in Incidence from PSA testing. The two peaks coincide (vertical green line connects the two charts at the peaks). Granted mortality declines afterwards, from 33,000 per year to 24,000 per year, but at a huge cost. We have eradicated 10,000 advanced prostate cancer cases per year in return for a huge price paid in degrading the quality of life for 1 million men overdiagnosed and overtreated for insignificant disease.
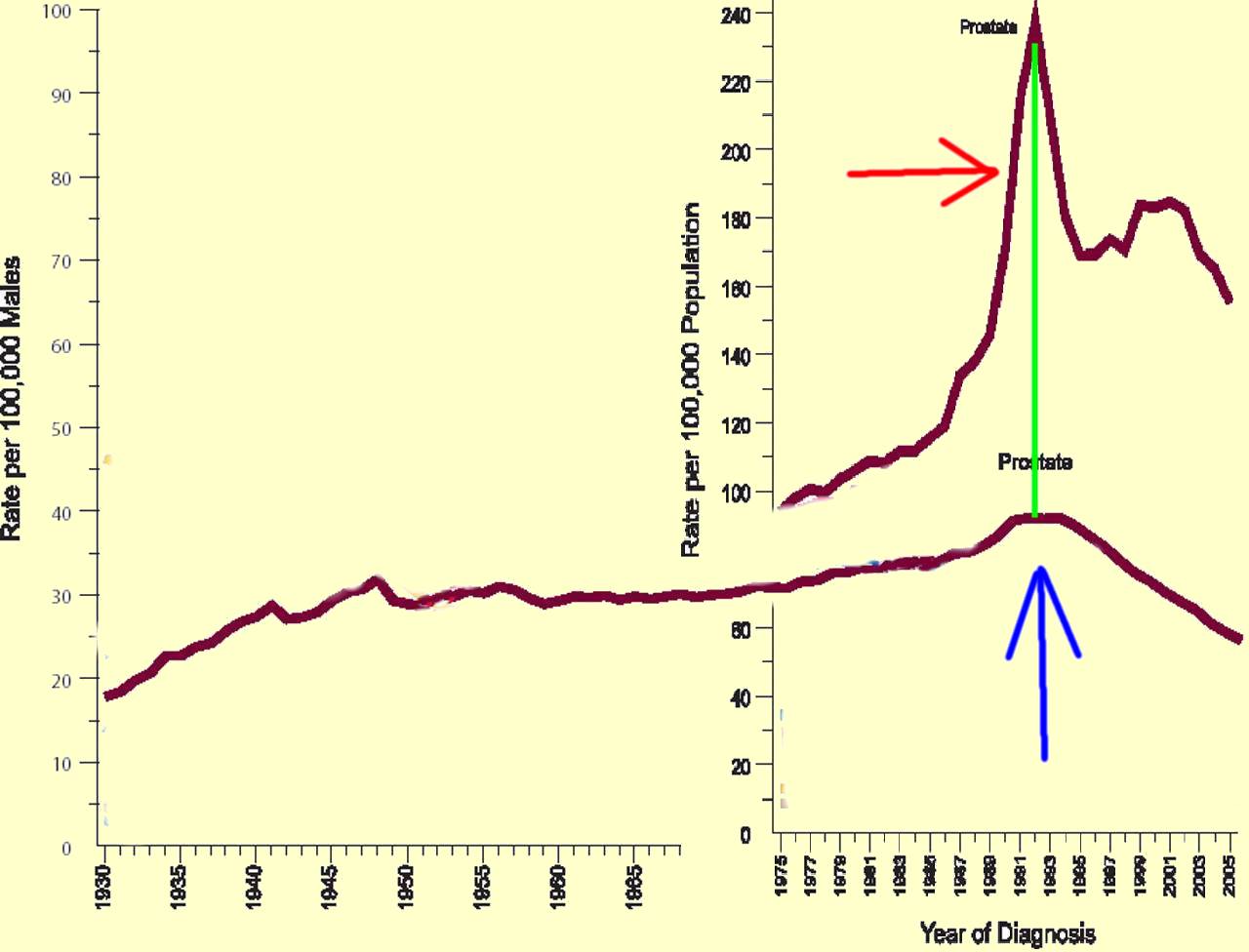 Source for above two charts: http://caonline.amcancersoc.org/cgi/content/full/59/4/225 Figure 3 and Figure 4 combined, FIGURE 3 Annual Age-adjusted Cancer Incidence Rates among Males and Females for Selected Cancers, United States, 1975– 2005. FIGURE 4 Annual Age-adjusted Cancer Death Rates among Males for Selected Cancers, United States, 1930–2005.
Source for above two charts: http://caonline.amcancersoc.org/cgi/content/full/59/4/225 Figure 3 and Figure 4 combined, FIGURE 3 Annual Age-adjusted Cancer Incidence Rates among Males and Females for Selected Cancers, United States, 1975– 2005. FIGURE 4 Annual Age-adjusted Cancer Death Rates among Males for Selected Cancers, United States, 1930–2005.
Another series of papers just released in the British Medical Journal Sept. 24 2009, again criticizes mass PSA screening, advising against it. Another highly critical article, just published in the Archives on Internal Medicine by Dr Kirsten Howard from the University of Sydney’s School of Public Health, showed that PSA Testing is not a major factor in prostate cancer mortality, and “many men with screen-detected prostate cancer are having cancer therapies for clinically insignificant cancers”.
 Left Image: Prostate diagnosis and treatment was rather barbaric during the middle ages. We have come a long way since then. Image of Die Saege.jpg courtesy of Wikimedia Commons.
Left Image: Prostate diagnosis and treatment was rather barbaric during the middle ages. We have come a long way since then. Image of Die Saege.jpg courtesy of Wikimedia Commons.
We have known since 1935 with the publication of Arnold Rich’s autopsy study that there is a large pool of latent, clinically insignificant prostate cancer in the male population which increases with age. By the age of fifty, 30-40 per cent of males will harbor a clinically insignificant focus of prostate cancer. The vast majority succumb to old age before the prostate cancer bothers them. These prostate cancers are the incidental findings at post mortem exam.
Prostate cancer is a slow growing indolent disease with a 99 per cent 5 year survival after diagnosis. The incidence of latent prostate cancer is estimated to be one half of the male population 65 and over (7 million of the 14 million males), yet there are only 30,000 deaths per year. This means the average male has a 0.5% chance of dying from prostate cancer, (or a 99.5 chance of dying from other causes, not prostate cancer).
PSA screening programs send the screened patients to trans-rectal ultrasound guided biopsy which finds these latent prostate cancers, many of which should not be treated. Mainstream conventional treatment involves radical prostatectomy, radiation therapy, or hormonal castration. The first two are associated with adverse effects of incontinence, and erectile dysfunction. Treatment with androgen blockade, (a form of chemical castration) is associated with increased mortality and osteoporosis.
One of the unmistakable impacts of wide scale PSA screening for prostate cancer has been the eradication of advanced cases over the past two decades. For example, during my training years in the nuclear medicine department at Rush Medical School in Chicago in the 1970’s, we followed dozens of patients with metastatic prostate cancer on serial bone scans. (see left image) This is rarely seen today. The advanced prostate cancer case is a rare bird driven to extinction, seen only occasionally.
Stephen Strum, MD, an oncologist from Oregon writes in this March 2009 NEJM article, “The nature of the patient diagnosed with PC has dramatically changed since the introduction of PSA in 1987. Almost gone are men presenting with advanced local or distant Prostate Cancer.”
Like the vanishing American Buffalo, these advanced metastatic prostate cancer cases have been hunted to the point of near extinction by the American PSA Screening Test.
 left Image: Vanishing Rare Bird, Metastatic Prostate Cancer Diagnosis. Bone Scan shows prostate cancer involving skeleton (bone metastasis, red arrows) courtesy of wikimedia commons.
left Image: Vanishing Rare Bird, Metastatic Prostate Cancer Diagnosis. Bone Scan shows prostate cancer involving skeleton (bone metastasis, red arrows) courtesy of wikimedia commons.
Stanford’s Dr. Thomas Stamey, the first to advocate PSA screening in 1987, has come full circle, and no longer recommends PSA screening. Stamey found the abundance of advanced cases from the early years of PSA Screening are gone, and the PSA test has become useless. Stamey declares, “The prostate specific antigen era in the United States is over for prostate cancer”.
 Left Image: American Buffalo hunted to near extinction. Courtesy of wikimedia commons.
Left Image: American Buffalo hunted to near extinction. Courtesy of wikimedia commons.
Stamey’s data shows there was a substantial decrease in correlation between PSA levels and the amount of prostate cancer – from 43 percent predictive ability in the first five-year group down to 2 percent in the most recent one. “Our job now is to stop removing every man’s prostate who has prostate cancer,” said Stamey. “We originally thought we were doing the right thing, but we are now figuring out how we went wrong.”
In 1997, the American Cancer Society changed its position and no longer recommends screening under the leadership of Otis Brawley MD, their chief Medical Officer who declined PSA screening for himself, personally. Otis Brawley, MD says.”twenty-three organizations of experts from the Canadian Urology Association to the American College of Physicians to the U.S. Preventive Services Task Force recommend against screening…the predominance of professional expert opinion is that (PSA screening) is unproven and should not be done.”
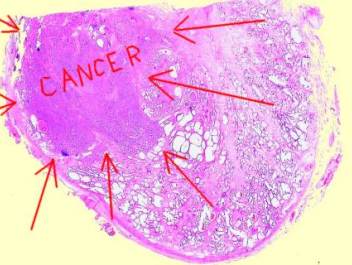 Above Image: Prostate cancer (red arrows) on histology slide courtesy of wikimedia commons.
Above Image: Prostate cancer (red arrows) on histology slide courtesy of wikimedia commons.
According to Dr Bicker’s August 2009 article in Anticancer Research, PSA is now commonly regarded as an indicator of prostate volume, and is not independently diagnostic or prognostic in prostate cancer. Even though mass screening of asymptomatic men with the PSA test is no longer recommended, the PSA test remains a very useful tool in the diagnosis and follow up of prostate cancer. For example, the PSA is useful as a cancer marker to follow cancer recurrence, progression or regression after treatment.
Gleason Score can help: Gleason Score is a histology grading pattern used to grade the biopsy sample. Lower scores (one and two at left of diagram) are associated with better prognosis. Higher scores (4 and 5 to right of diagram) are associated with worse prognosis with more aggressive behavior of the tumor. Diagram courtesy of Donald F Gleason MD PhD.
One of the major problems with prostate cancer screening with PSA, is the inability of this test to differentiate the clinically insignificant cancers that don’t require treatment from the dangerous cancers that do.
 Various authors have suggested refinements by using parameters such as PSA velocity, Free PSA ratio, and of course, the Gleason score, a form of histology grading, applied to prostate biopsy sample to provide this discrimination. Using these refinements, some doctors such as Laurence Klotz have advocated Active Surveillance based on PSA velocity. Dr Klotz offers treatment for cases having a PSA Doubling Time of 3 years or less (based on a minimum of three determinations over 6 months). Others, such as Mark Soloway MD, feel that Gleason score upgrade or histologic evidence of tumor aggression is the most important parameter, and have offered radical treatment if this is found at repeat biopsy. The obvious goal is to identify and treat aggressive tumors before they invade the prostatic capsule and beyond. This is not so simple and may require discovery of new biomarkers.
Various authors have suggested refinements by using parameters such as PSA velocity, Free PSA ratio, and of course, the Gleason score, a form of histology grading, applied to prostate biopsy sample to provide this discrimination. Using these refinements, some doctors such as Laurence Klotz have advocated Active Surveillance based on PSA velocity. Dr Klotz offers treatment for cases having a PSA Doubling Time of 3 years or less (based on a minimum of three determinations over 6 months). Others, such as Mark Soloway MD, feel that Gleason score upgrade or histologic evidence of tumor aggression is the most important parameter, and have offered radical treatment if this is found at repeat biopsy. The obvious goal is to identify and treat aggressive tumors before they invade the prostatic capsule and beyond. This is not so simple and may require discovery of new biomarkers.
A new bio-marker in prostate cancer cells called Hsp-27 protein indicates an aggressive type of prostate cancer that requires treatment. The absence of the Hsp-27 protein suggests a silent type of cancer that does not require immediate treatment.
Do these new protocols and tools work any better than the old ones? We don’t know yet. It may take another ten years to find out.
Given the reality that PSA screening for early detection for prostate cancer is a misguided adventure which leads to overdiagnoisis and does more harm than good, perhaps another approach to prevention is warranted. Such an approach is suggested by urologist Ronald Wheeler at the Sarosota Prostate Center. Dr Wheeler advocates a nutritional program for prostate cancer prevention with Vitamins C, B6, E, zinc, selenium, Saw palmetto, Pygeum africanum, stinging nettle, pumpkin seed, Echinacea purpurea, garlic, ginkgo biloba, Amino acids–L-glycine, L-alanine, L-glutamic acid and Modified Mediterranean Diet (link).
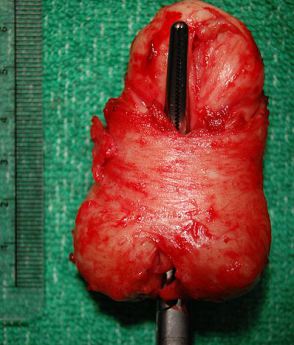 Left Image: Prostate specimen with median lobe hypertropy courtesy of wikimedia commons.
Left Image: Prostate specimen with median lobe hypertropy courtesy of wikimedia commons.
In 20 patients with biopsy proven prostate cancer who had declined radical treatment, Dr Wheeler’s herbal-nutritional supplement program reduced mean PSA from 6.8 ng/ml to 3.4 ng/ml over three years of follow-up. A detailed listing of patient PSA data from the study can be found on this page.
I would also add digestive enzymes, and optimizing vitamin D level with testing and supplementation, as well as optimizing Iodine levels with Iodoral would also be included in a typical prostate cancer prevention program.
Conclusion
In conclusion, PSA screening for prostate cancer has been a failed medical experiment leaving behind 1 million male victims treated unnecessarily for a type of prostate cancer that was clinically insignificant, providing little or no benefit in terms of lives saved. Leaders in the field are now alerting us to the pitfalls, harms and limitations involved in PSA cancer screening.
Recognizing that there are 30,000 prostate cancer deaths per year, the urgent challenge is to identify and treat the aggressive cancers destined to kill the host, and avoid harming the other 7 million men representing a silent reservoir of biologically insignificant disease. Hopefully, this will be the subject of future NIH funded research, so that another one million men in the future will be spared needless overdiagnosis and overtreatment.
Links to articles with related content:
Increased Mortality from Testosterone Blockade for Prostate Cancer
Testosterone and Prostate Cancer Myths and Misconceptions
Jeffrey Dach MD
7450 Griffin Road Suite 190
Davie, Fl 33314
954-792-4663
http://www.jeffreydach.com/
http://www.drdach.com/
http://www.naturalmedicine101.com/
http://www.truemedmd.com/
Links and References
http://www.nytimes.com/2009/03/19/health/19cancer.html
Prostate Test Found to Save Few Lives By GINA KOLATA NY Times Published: March 18, 2009
The findings, the first based on rigorous, randomized studies, confirm some longstanding concerns about the wisdom of widespread prostate cancer screening. Although the studies are continuing, results so far are considered significant and the most definitive to date.
The PSA test, which measures a protein released by prostate cells, does what it is supposed to do — indicates a cancer might be present, leading to biopsies to determine if there is a tumor. But it has been difficult to know whether finding prostate cancer early saves lives. Most of the cancers tend to grow very slowly and are never a threat and, with the faster-growing ones, even early diagnosis might be too late.
The studies — one in Europe and the other in the United States — are “some of the most important studies in the history of men’s health,” said Dr. Otis Brawley, the chief medical officer of the American Cancer Society.
In the European study, 48 men were told they had prostate cancer and needlessly treated for it for every man whose death was prevented within a decade after having had a PSA test.
Taken together, the studies found that screening was associated with a 20 percent relative reduction in the prostate cancer death rate. But the number of lives saved was small — seven fewer prostate cancer deaths for every 10,000 men screened and followed for nine years.
ONE MILLION MEN – Victims of PSA Screening
http://jnci.oxfordjournals.org/cgi/content/abstract/djp278v1
Prostate Cancer Diagnosis and Treatment After the Introduction of Prostate-Specific Antigen Screening: 1986–2005
H. Gilbert Welch, Peter C. Albertsen Journal of the National Cancer Institute Advance Access published online on August 31, 2009
Results: Overall incidence of prostate cancer rose rapidly after 1986, peaked in 1992, and then declined, albeit to levels considerably higher than those in 1986. Overall incidence, however, obscured distinct age-specific patterns: The relative incidence rate (2005 relative to 1986) was 0.56 in men aged 80 years and older, 1.09 in men aged 70–79 years, 1.91 in men aged 60–69 years, 3.64 in men aged 50–59 years, and 7.23 in men younger than 50 years. Since 1986, an estimated additional 1 305 600 men were diagnosed with prostate cancer, 1 004 800 of whom were definitively treated for the disease. Using the most optimistic assumption about the benefit of screening—that the entire decline in prostate cancer mortality observed during this period is attributable to this additional diagnosis—we estimated that, for each man who experienced the presumed benefit, more than 20 had to be diagnosed with prostate cancer.
Conclusions: The introduction of PSA screening has resulted in more than 1 million additional men being diagnosed and treated for prostate cancer in the United States. The growth is particularly dramatic for younger men. Given the considerable time that has passed since PSA screening began, most of this excess incidence must represent overdiagnosis.
http://www.medicinenet.com/script/main/art.asp?articlekey=105197
PSA Test: More Harm Than Good? Study: 1 Million Men Suffered Needless Treatment After Prostate Cancer Test By Daniel J. DeNoon WebMD Health News Aug. 31, 2009 — The PSA prostate cancer screening test does more harm than good, a new study suggests.
How much harm and how much good? “For every man who avoids a prostate cancer death due to PSA screening, about 50 men have to be treated unnecessarily — and a third of these men will have serious problems with treatment,” study co-author H. Gilbert Welch, MD, MPH, tells WebMD.
http://www.cnn.com/2009/HEALTH/09/01/prostate.cancer.screening/index.html
Study: Prostate cancer test leads to needless diagnoses
•Study: Many men do not benefit from a prostate cancer test called a PSA test
•PSA is a protein produced by cells of the prostate gland
•For one life saved, more than 20 are overdiagnosed
•There’s no clear consensus on screening from the major medical organizations
Tue September 1, 2009 By Denise Mann – More than one million American men may have been unnecessarily diagnosed and treated for prostate cancer since widespread use of the prostate-specific antigen (PSA) blood test began in 1987, a new study says.
http://www.modernmedicine.com/modernmedicine/Enews/Prostate-cancer-overdiagnosis-attributed-to-PSA-te/ArticleStandard/Article/detail/624305?contextCategoryId=40237&ref=25
Prostate cancer overdiagnosis attributed to PSA test – Sep 10, 2009 Urology Times E-News
Since its introduction in 1986, PSA screening has resulted in more than one million men being needlessly diagnosed and treated for prostate cancer, according to a study published online Aug. 31 in the Journal of the National Cancer Institute.
Using data from the National Cancer Institute’s Surveillance, Epidemiology, and End Results SEER program, researchers at the White River Junction VA, the Dartmouth Institute for Health Policy & Clinical Practice, and the University of Connecticut examined age-specific prostate cancer incidence rates from the U.S. Census to determine the excess or deficit in the number of men diagnosed and treated for prostate cancer each year since 1986.
According to the researchers, overall incidence of prostate cancer rose rapidly, peaked, and declined to levels considerably higher than in 1986. Regardless of age, an additional 1.3 million men were diagnosed who would otherwise not have been diagnosed without PSA screening, and more than one million have been treated since 1986.
“Given the considerable time that has passed since PSA screening began, most of this excess incidence must represent overdiagnosis,” the authors wrote. “All overdiagnosed patients are needlessly exposed to the hassle factors of obtaining treatment, the financial implications of the diagnosis, and the anxieties associated with becoming a cancer patient.”
The increased diagnosis has been most dramatic among younger men: more than tripling since 1986 in men aged 50 to 59 years (from 58.4 to 212.7 per 100,000) and more than a sevenfold increase in men under age 50 (from 1.3 to 9.4 per 100,000).
http://www.webmd.com/prostate-cancer/news/20090831/psa-test-more-harm-than-good
PSA Test: More Harm Than Good? Study: 1 Million Men Suffered Needless Treatment After Prostate Cancer Test By Daniel J. DeNoon WebMD Health News – Aug. 31, 2009 — The PSA prostate cancer screening test does more harm than good, a new study suggests. How much harm and how much good? “For every man who avoids a prostate cancer death due to PSA screening, about 50 men have to be treated unnecessarily — and a third of these men will have serious problems with treatment,” study co-author H. Gilbert Welch, MD, MPH, tells WebMD. The blood test detects prostate-specific antigen (PSA) in the blood. Rising PSA levels may, or may not, mean prostate cancer. So men with suspicious PSA levels undergo prostate biopsies.
http://www.baltimoresun.com/health/bal-md.hs.psa01sep01,0,7710170.story
Doubt cast on value of PSA test By Kelly Brewington- Baltimore Sun September 1, 2009
Study indicates prostate cancer indicator results in more harm than good. The findings, published in Monday’s Journal of the National Cancer Institute, found that since a blood test became the standard way to screen for prostate cancer, an additional 1.3 million men have been diagnosed with the disease. But because many men are diagnosed with cancer that will not cause symptoms and will not kill them, the screening tests save few lives, the authors conclude.
Adult Urology Prostate Specific Antigen Best Practice Statement: 2009 Update Kirsten L. Greene. Although recently published trials show different results regarding the impact of prostate cancer screening on mortality, both suggest that prostate cancer screening leads to overdetection and overtreatment of some patients. Therefore, men should be informed of the risks and benefits of prostate cancer screening before biopsy, and the option of active surveillance in lieu of immediate treatment for certain men diagnosed with prostate cancer.
Comment on Two NEJM studies by UCSF
http://synapse.ucsf.edu/articles/2009/March/26/prostate.html
Studies Cast Doubt on Value of Prostate Screenings Synapse Staff Report UCSF
Two major, long-awaited studies on prostate cancer were released on March 19, and both sharply questioned the conventional wisdom about treating the disease. According to the studies, screening men for prostate cancer provides little or no benefit in saving lives. Further, the studies contend that treatment of prostate cancer can be painful and embarrassing and not provide any significant health benefit. The screenings, known as the PSA blood test, indicates whether a cancer is present, leading to biopsies to determine if there is a tumor. But there has been much controversy over whether detecting prostate cancer early actually saves lives. The critics note that many prostate tumors grow so slowly that the patient is likely to die of other causes before the prostate cancer becomes a threat. The studes, one European and one American, were hailed as “some of the most important studies in the history of men’s health,” said Dr. Otis Brawley, the chief medical officer of the American Cancer Society.
NEJM March 2009 No Mortality Benefit of Screening
http://content.nejm.org/cgi/content/full/NEJMoa0810696
Volume 360:1310-1319 March 26, 2009 Number 13
Mortality Results from a Randomized Prostate-Cancer Screening Trial.
ABSTRACT. Background The effect of screening with prostate-specific–antigen (PSA) testing and digital rectal examination on the rate of death from prostate cancer is unknown. This is the first report from the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial on prostate-cancer mortality.
Methods: From 1993 through 2001, we randomly assigned 76,693 men at 10 U.S. study centers to receive either annual screening (38,343 subjects) or usual care as the control (38,350 subjects). Men in the screening group were offered annual PSA testing for 6 years and digital rectal examination for 4 years. The subjects and health care providers received the results and decided on the type of follow-up evaluation. Usual care sometimes included screening, as some organizations have recommended. The numbers of all cancers and deaths and causes of death were ascertained.
Results In the screening group, rates of compliance were 85% for PSA testing and 86% for digital rectal examination. Rates of screening in the control group increased from 40% in the first year to 52% in the sixth year for PSA testing and ranged from 41 to 46% for digital rectal examination. After 7 years of follow-up, the incidence of prostate cancer per 10,000 person-years was 116 (2820 cancers) in the screening group and 95 (2322 cancers) in the control group (rate ratio, 1.22; 95% confidence interval [CI], 1.16 to 1.29). The incidence of death per 10,000 person-years was 2.0 (50 deaths) in the screening group and 1.7 (44 deaths) in the control group (rate ratio, 1.13; 95% CI, 0.75 to 1.70). The data at 10 years were 67% complete and consistent with these overall findings.
Conclusions: After 7 to 10 years of follow-up, the rate of death from prostate cancer was very low and did not differ significantly between the two study groups.
——————————————————————————–
The benefit of screening for prostate cancer with serum prostate-specific–antigen (PSA) testing, digital rectal examination, or any other screening test is unknown. There has been no comprehensive assessment of the trade-offs between benefits and risks. Despite these uncertainties, PSA screening has been adopted by many patients and physicians in the United States and other countries. The use of PSA testing as a screening tool has increased dramatically in the United States since 1988.1 Numerous observational studies have reported conflicting findings regarding the benefit of screening.2 As a result, the screening recommendations of various organizations differ. The American Urological Association and the American Cancer Society recommend offering annual PSA testing and digital rectal examination beginning at the age of 50 years to men with a normal risk of prostate cancer and beginning at an earlier age to men at high risk.3,4 The National Comprehensive Cancer Network recommends a risk-based screening algorithm, including family history, race, and age.5 In contrast, the U.S. Preventive Services Task Force recently concluded that there was insufficient evidence in men under the age of 75 years to assess the balance between benefits and side effects associated with screening, and the panel recommended against screening men over the age of 75 years.6
NEJM European Study March 2009 -Mortality reduced 20% but high overdiagnosis rate. ERSPC
http://content.nejm.org/cgi/content/full/NEJMoa0810084
Volume 360:1320-1328 March 26, 2009 Number 13
Screening and Prostate-Cancer Mortality in a Randomized European Study
Fritz H. Schröder, M.D., Jonas Hugosson, M.D.,
ABSTRACT: Background The European Randomized Study of Screening for Prostate Cancer ERSPC was initiated in the early 1990s to evaluate the effect of screening with prostate-specific–antigen (PSA) testing on death rates from prostate cancer.
Methods: We identified 182,000 men between the ages of 50 and 74 years through registries in seven European countries for inclusion in our study. The men were randomly assigned to a group that was offered PSA screening at an average of once every 4 years or to a control group that did not receive such screening. The predefined core age group for this study included 162,243 men between the ages of 55 and 69 years. The primary outcome was the rate of death from prostate cancer. Mortality follow-up was identical for the two study groups and ended on December 31, 2006.
Results: In the screening group, 82% of men accepted at least one offer of screening. During a median follow-up of 9 years, the cumulative incidence of prostate cancer was 8.2% in the screening group and 4.8% in the control group. The rate ratio for death from prostate cancer in the screening group, as compared with the control group, was 0.80 (95% confidence interval [CI], 0.65 to 0.98; adjusted P=0.04). The absolute risk difference was 0.71 death per 1000 men. This means that 1410 men would need to be screened and 48 additional cases of prostate cancer would need to be treated to prevent one death from prostate cancer. The analysis of men who were actually screened during the first round (excluding subjects with noncompliance) provided a rate ratio for death from prostate cancer of 0.73 (95% CI, 0.56 to 0.90).
Conclusions PSA-based screening reduced the rate of death from prostate cancer by 20%
but was associated with a high risk of overdiagnosis.
European Study July 2009 Adjusted for contamination and non-attendance:
better results
http://www.ncbi.nlm.nih.gov/pubmed/19660851
Eur Urol. 2009 Jul 28. Prostate ancer Mortality Reduction by Prostate-Specific Antigen-Based Screening Adjusted for Nonattendance and Contamination in the European Randomised Study of Screening for Prostate Cancer (ERSPC). Roobol MJ, Kerkhof M, Schröder FH, Cuzick J, Sasieni P, Hakama M, Stenman UH, Ciatto S, Nelen V, Kwiatkowski M, Lujan M, Lilja H, Zappa M, Denis L, Recker F, Berenguer A, Ruutu M, Kujala P, Bangma CH, Aus G, Tammela TL, Villers A, Rebillard X, Moss SM, de Koning HJ, Hugosson J, Auvinen A. Department of Urology, Erasmus MC, Rotterdam, The Netherlands.
BACKGROUND: Prostate-specific antigen (PSA) based screening for prostate cancer (PCa) has been shown to reduce prostate specific mortality by 20% in an intention to screen (ITS) analysis in a randomised trial (European Randomised Study of Screening for Prostate Cancer [ERSPC]). This effect may be diluted by nonattendance in men randomised to the screening arm and contamination in men randomised to the control arm. OBJECTIVE: To assess the magnitude of the PCa-specific mortality reduction after adjustment for nonattendance and contamination.
DESIGN, SETTING, AND PARTICIPANTS: We analysed the occurrence of PCa deaths during an average follow-up of 9 yr in 162 243 men 55-69 yr of age randomised in seven participating centres of the ERSPC. Centres were also grouped according to the type of randomisation (ie, before or after informed written consent). INTERVENTION: Nonattendance was defined as nonattending the initial screening round in ERSPC. The estimate of contamination was based on PSA use in controls in ERSPC Rotterdam. MEASUREMENTS: Relative risks (RRs) with 95% confidence intervals (CIs) were compared between an ITS analysis and analyses adjusting for nonattendance and contamination using a statistical method developed for this purpose.
RESULTS AND LIMITATIONS: In the ITS analysis, the RR of PCa death in men allocated to the intervention arm relative to the control arm was 0.80 (95% CI, 0.68-0.96). Adjustment for nonattendance resulted in a RR of 0.73 (95% CI, 0.58-0.93), and additional adjustment for contamination using two different estimates led to estimated reductions of 0.69 (95% CI, 0.51-0.92) to 0.71 (95% CI, 0.55-0.93), respectively. Contamination data were obtained through extrapolation of single-centre data. No heterogeneity was found between the groups of centres.
CONCLUSIONS: PSA screening reduces the risk of dying of PCa by up to 31% in men actually screened. This benefit should be weighed against a degree of overdiagnosis and overtreatment inherent in PCa screening.
Sept 2009 BMJ Papers
http://blog.lib.umn.edu/schwitz/healthnews/2009/09/bmj-papers-conc-1.html
BMJ papers conclude there’s not enough evidence to support widespread PSA screening – By Gary Schwitzer on September 24, 2009 6:02 PM
At the end of prostate cancer awareness month – a promotion driven in large part by those who push prostate cancer screening and treatments – this week’s edition of the BMJ publishes a study, an analysis and an editorial all showing that there isn’t enough evidence to support population-wide prostate screening with the PSA blood test.
• The PSA test cannot show the difference between cancers that will kill and those that are harmless, leading to overdiagnosis and overtreatment of healthy men.
• The PSA test doesn’t produce the likelihood ratios (a measure used to predict disease) required for a screening test.
• Other tests – other biomarkers for early detection of prostate cancer are needed before population based screening for prostate cancer should be introduced.
• Until a better screening test is available, men and their doctors should use a shared decision making approach to discuss the harms and benefits and the uncertainties of prostate cancer screening.
• One excerpt from a Harvard analysis: “Given the current evidence, we support the opinion of the European Urological Association that data on costs and benefits remain insufficient to support population based screening. The financial and psychological costs of false positive results, overdiagnosis, and overtreatment of prostate cancer need to be measured more precisely. Better estimates of these costs should emerge from further evaluations of the large randomised trials.
Before testing men should be informed about the test itself and the interpretation of a positive or negative result. Moreover, they should be advised that the test cannot tell whether they have a life threatening cancer but that it could lead them through a thicket of tests and treatments that they might have better avoided. This advice follows the basic tenets of screening programmes laid out by the World Health Organization.”
BMJ Sept 2009
http://www.bmj.com/cgi/content/abstract/339/sep24_1/b3537
Published 24 September 2009, BMJ 2009;339:b3537
Prostate specific antigen for early detection of prostate cancer: longitudinal study.
Benny Holmström, urologist1,2, Mattias Johansson, postdoctoral fellow2,3, Anders Bergh, professor of pathology4, Ulf-Håkan Stenman, professor of clinical chemistry5, Göran Hallmans, professor of nutritional research6, Pär Stattin, professor of urology2
Conclusions: No single cut-off value for prostate specific antigen concentration attained likelihood ratios formally required for a screening test. Prostate specific antigen concentrations below 1.0 ng/ml virtually ruled out a prostate cancer diagnosis during the follow-up. Additional biomarkers for early detection of prostate cancer are needed before population based screening for prostate cancer should be introduced.
http://www.bmj.com/cgi/content/extract/339/sep24_1/b3601
Published 24 September 2009, BMJ 2009;339:b3601
Analysis Screening for prostate cancer remains controversial
Jennifer R Stark, postdoctoral fellow of epidemiology1,2, Lorelei Mucci, assistant professor of epidemiology1,2,5, Kenneth J Rothman, professor of epidemiology and medicine3,4, Hans-Olov Adami, professor of epidemiology1,5,6
http://www.bmj.com/cgi/content/extract/339/sep24_1/b3572
Published 24 September 2009, doi:10.1136/bmj.b3572
Cite this as: BMJ 2009;339:b3572
Editorials Prostate specific antigen for detecting early prostate cancer
Evidence is inconclusive, so patient education and shared decision making are essential
US News Watchful Waiting
Watchful Waiting Works for Older Men With Prostate Cancer, But experts stress the same does not hold true for patients under 60. Posted September 15, 2009
Consumer Reports Just Say NO
http://blogs.consumerreports.org/health/2009/09/
whats-wrong-with-free-prostatecancer-screening-yankees-psa-test-bat-for-the-cure-us-open-john-mcenro.html
September 14, 2009 More What’s wrong with free prostate-cancer screening?
At a New York Yankees game I went to last week, the team gave free Snoopy dolls to fans—and a charity offered free prostate-cancer screening to men age 40 and up. I’m sad to say I got there too late for one of the dolls. But I’m glad I passed on the blood test for prostate cancer.
http://medicalconsumers.org/2009/04/16/just-say-no-to-the-psa-prostate-cancer-test/
Just Say No to the PSA Prostate Cancer Test Posted by medconsumers on April 16, 2009
IN Favor of PSA Screening: Impact of PSA Screening –
Disappearance of Advanced and Metastatic Case Presentations
http://www.nejm.org/perspective-roundtable/screening-for-prostate-cancer/
Stephen Strum, MD, FACP Ashland, Oregon Physician — Oncologist 03/30/2009
PSA–Everything in Life is a two-edged sword. The nature of the patient diagnosed with PC has dramatically changed since the introduction of PSA in 1987.
Almost gone are men presenting with advanced local or distant PC. PSA has major benefits not only in diagnosis, but in the prevention, staging, and treatment of the entire spectrum of disease.
PSA inexpensive & non-invasive derivatives like doubling time, velocity, PSA density, free PSA percentage are important in understanding the nature of the PC: is it biologically aggressive or indolent? These tests are rarely used in my experience as an international consultant. When used and coupled with understanding the patient’s context of overall health and access to talented physicians, the cons of PSA testing diminish.
Refinements on PSA Test – Free PSA and PSA Velocity
Free PSA Test
http://www.psa-rising.com/prostatecancer/fpsa-flowchart.htm
The “free” PSA test (PSA-f) and how it may spare you a biopsy
The free PSA test, often written PSA-f or FPSA, sometimes called PSA II, helps your urologist decide whether you need a biopsy.
Low free PSA may indicate prostate cancer. High free PSA along with other factors may indicate that you have BPH and no need of biopsy.
The free PSA test measures the proportion of free PSA to bound PSA in the total PSA in your blood sample. It’s called this because PSA-f circulates in the bloodstream “unbound,” without a carrier protein.
Combined with prostate volume, percent free PSA calculation helps reduce the number of biopsies based on “false positive” PSA test results. This may spare you an unnecessary biopsy.
High free PSA — above 25% — usually indicates BPH (benign prostate hyperplasia).
Low free PSA likely signals prostate cancer. Most men with prostate cancer have a free PSA below 15%.
If free PSA is below 7%, prostrate cancer is most likely. According to American Cancer Society and National Cancer Institute, men with free PSA at 7% or lower should undergo biopsy. If biopsy is negative but free PSA remains low, repeat biopsy is in order.
If total PSA is low, rate of PSA rise over a series of tests may send a warning. PSA velocity is an independent measure of likely prostate cancer.
Chart PSA 2.5 to 10 Biopsy or free PSA test If percent free PSA is low >> BIOPSY
If percent free PSA is high (above 15%) repeat bood tests and rectal exam in a year.
PSA under 2.5 but more than .75 ng/ml higher than last year’s then biopsy.
PSA velocity
http://www.sciencedaily.com/releases/2007/05/070525074607.htm
Prostate Cancer: High Pretreatment PSA Velocity Predicts Worse Outcome ScienceDaily (May 25, 2007)
Calculating PSA velocity has shown promise as a prognostic indicator. Studies suggest that PSA velocity more than 2 ng/ml/year strongly suggests aggressive disease
“These findings,” conclude the authors, “highlight the ability of a pre-treatment PSA velocity > 2 ng/ml/year alone to identify men with aggressive prostate cancer and in whom effective systemic treatment in addition to mono-therapy with RP or RT is needed to decrease PCSM rates.”
Article: “Prostate Cancer-Specific Mortality After Radical Prostatectomy or External Beam Radiation Therapy in Men With 1 or More High-Risk Factors,” Anthony V D’Amico, Ming-Hui Chen, William J Catalona, Leon Sun, Kimberly A. Roehl, Judd W. Moul, CANCER; Published Online: May 25, 2007 (DOI: 10.1002/cncr. 22737); Print Issue Date: July 1, 2007.
http://www.drcatalona.com/quest/Summer04/quest_summer04_2.asp
PSA Velocity: Important New Tool in Fight Against Prostate Cancer – By William J. Catalona, MD Our study results indicate that men with a high PSA velocity should not be managed by “watchful waiting”, which could be especially harmful if the cancer is fast-growing. Our study suggests that a rapid rise in the PSA score is a sign the cancer is particularly aggressive, and some men with CaP and a high PSA Velocity will require more than a radical prostatectomy to prevent prostate cancer death.
“PSA Velocity will likely change the way Cancer of Prostate is diagnosed and treated.”
The results also imply that PSA velocity measurements during the year before the diagnosis of prostate cancer can help identify the potential aggressiveness of the cancers. Those with a .75 PSA increase within a year show a worrisome risk for prostate cancer. Those with a 2.0 increase within a year are more likely to have an aggressive cancer with a higher potential risk for death.
http://content.nejm.org/cgi/content/abstract/351/2/125
Volume 351:125-135 July 8, 2004 Number 2
Preoperative PSA Velocity and the Risk of Death from Prostate Cancer after Radical Prostatectomy Anthony V. D’Amico, M.D., Ph.D., Ming-Hui Chen, Ph.D., Kimberly A. Roehl, M.P.H., and William J. Catalona, M.D.
ABSTRACT
Background We evaluated whether men at risk for death from prostate cancer after radical prostatectomy can be identified using information available at diagnosis.
Methods We studied 1095 men with localized prostate cancer to assess whether the rate of rise in the prostate-specific antigen (PSA) level — the PSA velocity — during the year before diagnosis, the PSA level at diagnosis, the Gleason score, and the clinical tumor stage could predict the time to death from prostate cancer and death from any cause after radical prostatectomy.
Results As compared with an annual PSA velocity of 2.0 ng per milliliter or less, an annual PSA velocity of more than 2.0 ng per milliliter was associated with a significantly shorter time to death from prostate cancer (P<0.001) and death from any cause (P=0.01). An increasing PSA level at diagnosis (P=0.01), a Gleason score of 8, 9, or 10 (P=0.02), and a clinical tumor stage of T2 (P<0.001) also predicted the time to death from prostate cancer. For men with an annual PSA velocity of more than 2.0 ng per milliliter, estimates of the risk of death from prostate cancer and death from any cause seven years after radical prostatectomy were also influenced by the PSA level, tumor stage, and Gleason score at diagnosis.
Conclusions Men whose PSA level increases by more than 2.0 ng per milliliter during the year before the diagnosis of prostate cancer may have a relatively high risk of death from prostate cancer despite undergoing radical prostatectomy.
psa velocity NOT Useful to determine biospy
Prostate Cancer
Prostate-Specific Antigen Velocity for Early Detection of Prostate Cancer: Result from a Large, Representative, Population-based Cohort
Andrew J. Vickersa, , , Tineke Woltersd, Caroline J. Savagea, Angel M. Cronina, M. Frank O’Briena, Kim Petterssonc, Monique J. Roobold, Gunnar Ausb, Peter T. Scardinoa, Jonas Hugossonb, Fritz H. Schröderd and Hans Liljaa, e
Conclusions: In men with PSA of about ≥3 ng/ml, we found little justification for formal calculation of PSAV or for use of PSAV cut points to determine biopsy. Informal assessment of PSAV will likely aid clinical judgment, such as a sudden rise in PSA suggesting prostatitis, which could be further evaluated before biopsy.
PSA is Good Predictor of Prostate Volume
http://www.ncbi.nlm.nih.gov/pubmed/10096388
Urology. 1999 Mar;53(3):581-9
Serum prostate-specific antigen as a predictor of prostate volume in men with benign prostatic hyperplasia. Roehrborn CG et al. Conclusions. Prostate volume is strongly related to serum PSA in men with BPH and no evidence of prostate cancer, and the relationship depends on age.
PSA elevation Caused by Bacterial Infection – RX CIPRO
http://www.ncbi.nlm.nih.gov/pubmed/15947609?dopt=Abstract
J Urol. 2005 Jul;174(1):161-4.
Treatment of chronic bacterial prostatitis with levofloxacin and ciprofloxacin lowers serum prostate specific antigen. Schaeffer AJ, Wu SC, Tennenberg AM, Kahn JB.
PURPOSE: We compared baseline and post-therapy prostate specific antigen (PSA) in patients with chronic bacterial prostatitis who were treated with levofloxacin or ciprofloxacin. MATERIALS AND METHODS: Subset analysis was done using a randomized, multicenter, double-blind, active control trial of 500 mg levofloxacin daily for 28 days vs 500 mg ciprofloxacin twice daily in 28 days in men with chronic bacterial prostatitis.
RESULTS: Of the 377 men in the intent to treat population, including 197 treated with levofloxacin and 180 treated with ciprofloxacin, 35 on levofloxacin and 37 on ciprofloxacin with baseline PSA greater than 4 ng/ml were included in this analysis. Excluded from analysis were 2 levofloxacin treated patients with extremely high PSA at baseline (62 and 103 ng/ml, respectively).
Mean baseline PSA +/- SD in the patients analyzed was 8.33 +/- 4.46 ng/ml, which decreased to 5.36 +/- 3.82 ng/ml after therapy.
CONCLUSIONS: Approximately 20% of patients diagnosed with chronic bacterial prostatitis had increased PSA. A significant decrease in PSA was observed in these patients after treatment with levofloxacin or ciprofloxacin. .
http://www.ncbi.nlm.nih.gov/pubmed/15693428
Arch Ital Urol Androl. 2004 Dec;76(4):154-8. PSA decrease after levofloxacin therapy in patients with histological prostatitis. Guercio S et al.
RESULTS: A total of 26 outpatients were evaluated (median age = 65 years). Median total serum PSA concentrations, before and after LVX therapy, were 7.1 ng/ml (range 4.1-15 ng/ml) and 5.8 ng/ml (2-15 ng/ml), respectively (p= n.s). The median reduction of total PSA was 16.6% (range 5.7 – 63.6%).
CONCLUSIONS: Treatment with LVX significantly reduced PSA values in over half of the patients with asymptomatic prostatitis, elevated total PSA and normal DRE and urinalysis. This approach could be applied in the ambulatory setting in order to increase the specificity of total PSA testing, reducing the number of negative, unnecessary, prostate biopsies.
http://www.ncbi.nlm.nih.gov/pubmed/11912396
J Urol. 2002 Apr;167(4):1723-6
Treatment of chronic prostatitis lowers serum prostate specific antigen. Bozeman CB et al.
PURPOSE: We evaluated men with documented chronic prostatitis and elevated serum prostate specific antigen (PSA) to determine whether treatment with antibiotics and anti-inflammatory drugs lowers serum PSA.
MATERIALS AND METHODS: We retrospectively reviewed the records of 95 men who presented with serum PSA greater than 4 ng./ml. and were subsequently diagnosed with chronic prostatitis with greater than 10 white blood cells per high power field in expressed prostatic excretions. Patients meeting these criteria were treated with a 4-week course of antibiotics and a nonsteroidal anti-inflammatory agent. In all patients followup PSA was determined within 2 months of treatment.
RESULTS: Mean PSA decreased 36.4% from 8.48 ng./ml. before to 5.39 after treatment (p <0.001). In 44 patients (46.3%) serum PSA decreased to below 4 ng./ml. (mean 2.48) and these patients no longer had an indication for biopsy. In the remaining 51 patients serum PSA remained elevated at greater than 4 ng./ml. and they underwent double sextant transrectal ultrasound guided biopsy. Pathological study showed prostate cancer in 13 cases (25.5%), chronic inflammation in 37 (72.5%) and only benign prostatic hypertrophy in 1 (1.05%). PSA in the 13 patients with prostate cancer decreased with treatment only 4.8% from 8.32 to 7.92 ng./ml. (p >0.05). Followup PSA at a mean of 11.4 months was determined in 19 of the 44 men who responded to treatment. Mean PSA increased only 4.5% from 2.35 to 2.46 ng./ml. (p >0.05) during this followup interval.
CONCLUSIONS: In almost half of the patients diagnosed with elevated PSA and chronic prostatitis serum PSA normalized with treatment and there was no longer an indication for transrectal ultrasound guided biopsy. Our study suggests that chronic prostatitis is an important cause of elevated PSA and when it is identified, treatment can decrease the percent of negative biopsies.
http://www.ncbi.nlm.nih.gov/pubmed/17695414
Arch Ital Urol Androl. 2007 Jun;79(2):84-92.
Reduction of PSA values by combination pharmacological therapy in patients with chronic prostatitis: implications for prostate cancer detection. Magri V et al,
We identified from our clinical database a total of 471 patients with PSA > or =4 ng/mL, were subjected to a 6-week course of 500 mg/day ciprofloxacin, 500 mg/day azithromycin (3 days/week), 10 mg/day alfuzosin and 320 mg b.i.d. Serenoa repens extract.
In summary, combination pharmacological therapy decreased the number of patients undergoing prostatic biopsy from 111 to 45. Normalization of PSA values in 59.4% of patients–not subjected to biopsy–increased the prostate cancer detection rate from 12.6% (14/111) to 31.1% (14/45).
http://www.ncbi.nlm.nih.gov/pubmed/17637759
Prostate Cancer Prostatic Dis. 2008;11(2):148-52. Epub 2007 Jul 17.
PSA reduction (after antibiotics) permits to avoid or postpone prostate biopsy in selected patients. Serretta V et al.
Microscopic foci of prostatitis may induce prostate-specific antigen (PSA) increase. PSA reduction after antibiotics might identify those patients in whom biopsy can be avoided. Ninety-nine patients received ciprofloxacin for 3 weeks, of whom 59 showed PSA reduction. Histology detected small foci of prostatitis in 65% of cases. Carcinoma was found in 40 and 20.3% of patients with unchanged or decreased PSA, respectively (P=0.03). No cancer was detected if PSA decreased below 4 ng/ml or more than 70%. Biopsy can be postponed, with a low risk of missing a cancer, if PSA decreases more than 70% or below 4 ng/ml.
_________
http://psg-mac43.ucsf.edu/ticr/syllabus/courses/26/2004/03/11/Lecture/readings/psa.pdf
Surrogate End Point for Prostate Cancer–Specific Mortality After Radical Prostatectomy or Radiation Therapy Anthony V. D’Amico, Judd W. Moul, Peter R. Carroll, Leon Sun, Deborah Lubeck,Ming-Hui Chen
http://www.ncbi.nlm.nih.gov/pubmed/17530618
Cancer. 2007 Jul 1;110(1):56-61. Prostate cancer-specific mortality after radical prostatectomy or external beam radiation therapy in men with 1 or more high-risk factors.
D’Amico AV, Chen MH, Catalona WJ, Sun L, Roehl KA, Moul JW.
Department of Radiation Oncology, Brigham and Women’s Hospital and Dana Farber Cancer Institute, Boston, Massachusetts 02215, USA.
BACKGROUND: Estimates of prostate cancer-specific mortality (PCSM) were determined after radical prostatectomy (RP) or radiation therapy (RT) in men with >or=1 high-risk factors. METHODS: The study cohort comprised 948 men who underwent RP (N = 660) or RT (N = 288) for localized prostate cancer between 1988 and 2004 and had at least 1 of the following high-risk factors: a prostate-specific antigen (PSA) velocity >2 ng/mL/year during the year before diagnosis, a biopsy Gleason score of >or=7, a PSA level of >or=10 ng/mL, or clinical category T2b or high disease. Grays regression was used to evaluate whether the number and type of high-risk factors were associated with time to PCSM. RESULTS: Multiple determinants of high risk were found to be significantly associated with a shorter time to PCSM after RP (P < .001) or RT (P <or= .001). The solitary presence of a PSA velocity >2 ng/mL/year was associated with an increased risk of PCSM after RP (hazards ratio [HR] of 7.3; 95% confidence interval [95% CI], 1.0-59 [P = .05]) or RT (HR of 12.1; 95% CI, 1.4-105 [P = .02]) when compared with men with any other single high-risk factor.
CONCLUSIONS: Men with a PSA velocity >2 ng/mL/year had a significantly higher risk of PCSM compared with men who had any other single high-risk factor. These men should be considered for randomized trials evaluating the impact on PCSM from adding systemic agents to standards of care for men with high-risk PC.
New Molecular Markers for Prostate CA in the Post PSA Era
http://www.ncbi.nlm.nih.gov/pubmed/19661347
Anticancer Res. 2009 Aug;29(8):3289-98. New molecular biomarkers for the prognosis and management of prostate cancer–the post PSA era. Bickers B, Aukim-Hastie C.
School of Pharmacy & Biomedical Sciences, University of Portsmouth, Portsmouth, Hampshire PO12DT, UK.
The widespread use of the PSA test has led to increased detection of the disease at earlier stages and a reduction in the number of patients where metastatic disease is found at diagnosis. However, there are significant limitations to the PSA test such as its lack of specificity, elevation in benign disease and failure to detect a significant number of PSA-negative tumours.
Therefore, PSA is now commonly regarded as an indicator of prostate volume and is not independently diagnostic or prognostic in prostate cancer. Due to these limitations, there is an urgent need for new prognostic biomarkers to enhance the clinical management of prostate cancer. There have been many recent advances in high-throughput technologies for measuring gene and protein expression in minimally invasive samples (e.g. blood, urine) that could more accurately predict disease progression. This review article gives a brief overview of biomarkers that are currently showing prognostic potential in prostate cancer research
Hsp-27
http://www.sciencedaily.com/releases/2009/09/090923102335.htm
Two-Thirds Of Prostate Cancer Patients Do Not Need Treatment, Study Reveals
ScienceDaily (Sep. 24, 2009) — Research at the University of Liverpool involving more than 500 prostate cancer patients has revealed two thirds of cases did not require urgent treatment, due to the absence of a protein that indicates progressive disease.
In the largest study of its kind, the international team of pathologists studied an initial 4,000 prostate cancer patients over a period of 15 years
Pathologists found that the presence of a protein, called Hsp-27, in cancer cells was an indicator that the disease will progress and require treatment. The study showed, however, that in more than 60% of cases the protein was not expressed and the cancer could be managed by careful monitoring, rather than with active invention methods, such as drug treatment or surgery.
http://www.nature.com/bjc/journal/vaop/ncurrent/abs/6605227a.html
http://www.ncbi.nlm.nih.gov/pubmed/19707199
Br J Cancer. 2009 Aug 25. [Epub ahead of print]
Hsp-27 expression at diagnosis predicts poor clinical outcome in prostate cancer independent of ETS-gene rearrangement. Foster CS et al
Background: This study was performed to test the hypothesis that expression of small heat shock protein Hsp-27 is, at diagnosis, a reliable predictive biomarker of clinically aggressive prostate cancer.
Methods:A panel of tissue microarrays constructed from a well-characterised cohort of 553 men with conservatively managed prostate cancer was stained immunohistochemically to detect Hsp-27 protein. Hsp-27 expression was compared with a series of pathological and clinical parameters, including outcome.
Results:Hsp-27 staining was indicative of higher Gleason score (P<0.001). In tissue cores having a Gleason score >7, the presence of Hsp-27 retained its power to independently predict poor clinical outcome (P<0.002). Higher levels of Hsp-27 staining were almost entirely restricted to cancers lacking ERG rearrangements (chi(2) trend=31.4, P<0.001), although this distribution did not have prognostic significance.
Interpretation:This study has confirmed that, in prostate cancers managed conservatively over a period of more than 15 years, expression of Hsp-27 is an accurate and independent predictive biomarker of aggressive disease with poor clinical outcome (P<0.001).
ASA and NSAIDS Lowers PSA
http://www.sciencedaily.com/releases/2008/11/081116142322.htm
Men Who Take Aspirin Have Significantly Lower PSA Levels
ScienceDaily (Nov. 17, 2008) — The use of aspirin and other non-steroidal anti-inflammatory drugs (NSAIDs) is significantly associated with lower PSA levels, especially among men with prostate cancer, say researchers at Vanderbilt University.
http://www.sciencedaily.com/releases/2008/05/080515072654.htm
Low Cholesterol Leads To Lower PSA, Lower Prostate Cancer Risk, Study Suggests
ScienceDaily (May 18, 2008) — Managing your cholesterol may also help you manage your prostate- specific antigen (PSA) level. Data presented at the 103rd Annual Scientific Meeting of the American Urological Association explored the relationship between low-density lipoprotein (LDL) cholesterol and PSA prior to beginning statin therapy.
Dr Catalona
http://www.drcatalona.com/quest/Spring04/quest_spring04_1.asp
The measurement of PSA, what is called the total PSA (tPSA), is not as accurate a detector of prostate cancer as doctors or patients would hope because PSA levels can also be elevated with benign conditions such as BPH (benign prostatic hyperplasia), prostatitis, recent ejaculation and minor trauma to the prostate by digital rectal examination, catheterization, or urinary retention.
Prostate cancer is more likely to be present if the ratio of free PSA to total PSA is less than 15%; therefore, low free PSA values are more likely to be associated with prostate cancer than high free PSA values.These compared measurements of free PSA and complexed PSA improve the ability to tell whether a rising PSA is from cancer or benign prostatic disease.
The percent of fPSA in blood is increased in men with BPH because the inner portion (transition zone) of the prostate, where BPH predominantly occurs, contains elevated levels of certain forms of fPSA that leak into the bloodstream but aren’t naturally there otherwise.
Pro-PSA
Prostate cancer, on the other hand, develops predominantly within the peripheral zone of the prostate gland.
Studies from this area reveal another form of PSA, called proPSA, which is elevated in cancerous prostate tissue. For reasons still unknown, pro-PSA accumulates in the tumor.
Pro-PSA has many forms. One, [-2]pro-PSA, has received the most clinical attention because it has been the primary form found in tumor samples.
The ratio of pro-PSA to free PSA has been shown in preliminary studies to be a most effective predictor of cancer in patients with total PSA levels in the 2.6-4 range and works almost as well in the 4 to 10 range.
If these studies are verified, pro-PSA levels might be preferable to free or complexed PSA as a clinical marker for cancer.
With greater acceptance and use of lower PSA cutoffs, more men will be advised to have biopsies and then pro-PSA markers could serve to eliminate unnecessary biopsies.
PSA Velocity
PSA velocity measures the rate of change of PSA as a function of time. An increase in the PSA level of 0.75 ng/mL per year has been reported to be suspicious for prostate cancer.
http://cancer.suite101.com/article.cfm/accuracy_of_psa_tests
Accuracy of PSA Tests Many Factors Elevate and Lower PSA Results
Steve Vogel Oct 31, 2008
Evidence Against PSA Screening for Prostate CA
http://www.themedguru.com/20090926/newsfeature/
studies-highlight-inefficacy-psa-test-86128398.html
Studies highlight inefficacy of PSA test by Jyoti Pal – September 26, 2009 London, September 26: Findings of two new studies suggest that screening all men for prostate cancer using prostate specific antigen (PSA), a common blood test used to detect the disease, is superfluous
PSA does not distinguish lethal and innocuous cancers. Dr. Mattias Johansson of the International Agency for Research on Cancer in Lyon, France and co-author of one of the studies averred, “In particular, tools that help distinguish rapidly growing and potentially lethal tumors from slow growing tumors are warranted in order to minimize over diagnosis and over treatment.”
Benny Holmstrom, a urologist with Gavle Hospital in Gavle, Sweden, and lead author of the study noted, “Our findings strongly indicate that, in addition to PSA, further biomarkers are needed before inferring population-based screening for prostate cancer.”
http://www.medpagetoday.com/Urology/ProstateCancer/16142
No Evidence to Support Routine PSA Screening, By Chris Emery, Contributing Writer, MedPage Today, Published: September 25, 2009 Reviewed by Zalman S. Agus, MD; Emeritus Professor University of Pennsylvania School of Medicine and Dorothy Caputo, MA, RN, BC-ADM, CDE, Nurse Planner
http://caonline.amcancersoc.org/cgi/content/full/59/4/220
Editorial – Prostate Cancer: Current Evidence Weighs Against Population Screening
Peter Boyle, PhD, DSc1 and Otis W. Brawley, MD2 . Published online before print June 29, 2009
CA Cancer J Clin 2009; 59:220-224
ERSPC and PLCO
Overdiagnosis and the resultant overtreatment and significant adverse events have been clearly established as a result of screening. Notably, in the ERSPC, screening the 73,000 men in the screened group resulted in >17,500 biopsies being performed to find a total of >5,900 prostate cancers. These figures are considerably higher than those in the unscreened group. Men in the screened group were 2.77 times more likely than those in the control group to undergo a radical prostatectomy and were twice as likely to receive radiation therapy.
Therapy for localized prostate cancer is not without its adverse effects, and undoubtedly many men suffered impotence, incontinence, and other complications as a result of this overtreatment. It is essential to have more information concerning the occurrence of such adverse events in these trials. The ERSPC concluded that it was necessary to screen 1,410 men and to have an additional 48 cancers diagnosed to prevent 1 prostate cancer death with a median follow–up of 9 years.12
In addition, it is concerning that in the PLCO study, the risk of death from all causes combined appeared to be higher in the screened group than in the control group. This is a weak observation, but it has been observed in 2 previous randomized trials. It raises the possibility that it could be due to a small increased risk of non–prostate cancer death from prostate cancer treatment. It has been reported that hormonal therapies in men with locoregional prostate cancer with gonadotropin–releasing hormone analogs increase the risk of diabetes, cardiovascular disease, and stroke.17 In the absence of details concerning treatment in these trials, it is not known how many of these men were treated with these drugs, but it needs to be ruled out that treatment may be harmful.
If one is to accept the ERSPC finding that screening decreases the risk of prostate cancer death by 20%, one must also accept the other findings of this trial. Forty-eight additional men were diagnosed in the screening group to save 1 life. This means an average man who gets screened is 48 times more likely to be harmed by screening than he is to be saved by screening at 9 years after diagnosis. The harms include that he may be diagnosed, undergo needless treatment, and suffer the side effects of prostate cancer treatment, which can include impotence, incontinence, mental anguish, and even death.
PSA screening not recommended for the elderly
http://jama.ama-assn.org/cgi/content/abstract/296/19/2336
PSA Screening Among Elderly Men With Limited Life Expectancies
Louise C. Walter, MD; Daniel Bertenthal, MPH; Karla Lindquist, MS; Badrinath R. Konety, MD
JAMA. 2006;296:2336-2342.
http://www.jurology.com/article/S0022-5347(08)03280-1/abstract
Volume 181, Issue 4, Pages 1606-1614 (April 2009) 27 of 126
Prostate Specific Antigen Testing Among the Elderly—When To Stop? Edward M. Schaeffera et al.
Clinical Utility of PSA Test
http://www.bmj.com/cgi/content/extract/339/sep22_1/b3527
Published 22 September 2009, doi:10.1136/bmj.b3527
Cite this as: BMJ 2009;339:b3527
Clinical Review Serum tumour markers: how to order and interpret them
C M Sturgeon, consultant clinical scientist1, L C Lai, professor of clinical biochemistry and metabolic medicine2, M J Duffy, professor of pathology and laboratory medicine3,4
Prostate specific antigen (PSA) may be used for detecting disease recurrence and monitoring treatment in patients with prostate cancer.
_______________
NEW Prostate Screen Studies
http://www.ccjm.org/content/76/8/446.full
The new data on prostate cancer screening: What should we do now? by TIMOTHY GILLIGAN, MD, MS. Similarly, there is growing interest in active surveillance for clinically localized low- or intermediate-grade prostate cancers, thus sparing men unnecessary and aggressive treatment.8 The challenge is determining which cancers are indolent and which are aggressive. Until we have accurate tools to make such a distinction, overtreatment will remain a problem as men and their doctors opt for aggressive treatment in the face of uncertainty about a cancer’s true danger.
REFERENCES
1.↵Klein E. What’s new in prostate cancer screening and prevention? Cleve Clin J Med 2009; 76:439–445.Abstract/FREE Full Text
2.↵Schröder FH, Hugosson J, Roobol MJ, et al.Screening and prostate-cancer mortality in a randomized European study. N Engl J Med 2009; 360:1320–1328.Abstract/FREE Full Text
3.↵Andriole GL, Crawford ED, Grubb RL, 3rd, et al.Mortality results from a randomized prostate-cancer screening trial. N Engl J Med 2009; 360:1310–1319.Abstract/FREE Full Text
4.↵Stanford JL, Stephenson RA, Coyle LM, et al.Prostate Cancer Trends 1973–1995. Bethesda, MD: National Cancer Institute; 1999.
5.↵Horner MJ, Ries LAG, Krapcho M, et al., editors. SEER Cancer Statistics Review, 1975–2006. Bethesda, MD: National Cancer Institute; 2009.
6.↵Sakr WA, Grignon DJ, Crissman JD, et al.High grade prostatic intraepithelial neoplasia (HGPIN) and prostatic adenocarcinoma between the ages of 20–69: an autopsy study of 249 cases. In Vivo 1994; 8:439–443.
7.↵Thompson IM, Goodman PJ, Tangen CM, et al.The influence of finasteride on the development of prostate cancer. N Engl J Med 2003; 349:215–224.
8.↵Klotz L. Active surveillance for favorable-risk prostate cancer: who, how and why? Nat Clin Pract Oncol 2007; 4:692–698.CrossRefMedline
===================
Autopsy Studies Showing Latent Prostate CA
http://www.ncbi.nlm.nih.gov/pubmed/108001
Classics in oncology. On the frequency of occurrence of occult carcinoma of the prostate: Arnold Rice Rich, M.D., Journal of Urology 33:3, 1935.
http://www.ncbi.nlm.nih.gov/pubmed/7803731
In Vivo. 1994 May-Jun;8(3):439-43. High grade prostatic intraepithelial neoplasia (HGPIN) and prostatic adenocarcinoma between the ages of 20-69: an autopsy study of 249 cases. Sakr WA et al.
Our results are summarized as follows: Seventy seven percent of the prostates with HGPIN harbored adenocarcinoma, whereas the frequency of cancer in prostates without HGPIN was 24%. HGPIN was encountered in 0, 5, 10, 41 and 63% of men in the 3rd, 4th, 5th and 7th decades, respectively. The corresponding figures for invasive carcinoma were 2, 29, 32, 55, and 64% respectively.
http://www.ncbi.nlm.nih.gov/pubmed/12518329
Prostate. 2003 Feb 15;54(3):238-47. Prevalence of prostate cancer and prostatic intraepithelial neoplasia in Caucasian Mediterranean males: an autopsy study. Sánchez-Chapado M et al.
RESULTS: Prevalence of Ca Prostate is 3.58, 8.82, 14.28, 23.80, 31.7, and 33.33% in the 3rd, 4th, 5th, 6th, 7th, and 8th decades, respectively. The rates of HGPIN were 7.14, 11.75, 35.71, 38.06, 45.40, and 48.15% at the 3rd, 4th, 5th, and 8th decades of life. Both CaP and HGPIN are located preferentially at the peripheral zone of the gland and in 21/27 cases (77.7%), an association between CaP and HGPIN was found.
http://www.ncbi.nlm.nih.gov/pubmed/16203079
Eur Urol. 2005 Nov;48(5):739-44. Epub 2005 Sep 15. The prevalence of prostate carcinoma and its precursor in Hungary: an autopsy study. Soos G, Tsakiris I, Szanto J, Turzo C, Haas PG, Dezso B. Department of Pathology, University of Debrecen, Medical and Health Science Centre, Debrecen, Hungary.
RESULTS: We found a 38.8% prevalence of incidental PCa with increasing age-related incidence. Both PCa and HGPIN are first detected in the 3rd decade and show a steady increase with age with respect to number of foci, tumor grade and volume. In the age group 81-95, 86.6% and 60% of men had PCa and HGPIN, respectively.
http://www.ncbi.nlm.nih.gov/pubmed/6154966
Scand J Urol Nephrol. 1980;14(1):29-35.Related Articles, Links
Latent prostatic cancer in a consecutive autopsy series. Hølund B.
In a consecutive series of autopsies, 223 prostates were removed. Latent prostatic cancer (LPC) was found in 50 cases (22%). All the tumours were adenocarcinomas. The frequency increased with age. No conclusive evidence was found of a relationship between prostatic hyperplasia and LPC. The extent of the tumour seemed to have greater prognostic significance than the degree of differentiation.
http://www.ncbi.nlm.nih.gov/pubmed/7107064?dopt=Abstract
1: Int J Cancer. 1982 Jun 15;29(6):611-6.Related Articles, Links
Geographic pathology of latent prostatic carcinoma. Yatani R, Chigusa I, Akazaki K, Stemmermann GN, Welsh RA, Correa P.
Prostates obtained at autopsy and examined microscopically. The age-adjusted overall prevalence of latent carcinoma was significantly higher in US blacks (36.9%), in US whites (34.6%) and in Colombians (31.5%) than in Japanese in Japan (20.5%). These results suggest that LNT tumors probably remain latent during the individual’s life span.
http://www.ncbi.nlm.nih.gov/pubmed/19077395
Urol Int. 2008;81(4):379-82. Epub 2008 Dec 10
Do clinically insignificant tumors of the prostate exist? Stamatiou K, Alevizos A, Mariolis A, Spiliopoulou C, Alevizou A, Bovis K, Sofras F. Department of Urology, University of Crete, School of Medicine, Heraklion, Greece.
CONCLUSIONS: The majority of impalpable PCs were low-volume, well-differentiated tumors corresponding to clinically insignificant neoplasms. Similar characteristics could be attributed to most of the impalpable carcinomas detected after prostatectomy in clinical practice.
PSA Leads to OverDiagnosis, and Unneccessary Detection and Treatment
http://ije.oxfordjournals.org/cgi/content/full/36/2/282
Commentary: Implications of the frequent occurrence of occult carcinoma of the prostate
Anthony B Miller, 13 November 2006.
About half of the men who die at the age of 70 or more have occult prostate cancer detectable at autopsy, while around 10–30% of men have these lesions at the age of 50–54,5 and about 30% of men harbour unsuspected prostate cancer by the end of the fifth decade of life.7 Some have suggested that if men lived to 150, nearly all will have them
Many have claimed that the large majority of lesions detected following a positive PSA test have all the features of malignancy, and inferred that if these lesions were not treated, they would eventually kill the patient. This is often used as a justification for PSA screening, and increasingly men are surviving who are convinced, that but for the PSA test, they would be dead by now—a belief often buttressed by their urologists, who use the argument to offset, and minimize, the distress caused by the consequences of treatment—impotence and incontinence. The possibility that the detection and treatment of the cancer, and more so the undesired consequences of such treatment was entirely unnecessary, is swept aside and ignored. But we have no right to ignore such possibilities, so it is right to review the evidence that confirms that the PSA test does result in what we term overdiagnosis, and thus unnecessary detection and treatment, as initially inferred was likely through the studies of Rice and his successors.
Free (no cost) PSA Screening Programs
http://prostate-cancer-questions-and-answers.com/2009/09/miami-urology-psa-test/
Miami urology doctors are offering a free PSA Test and DRE exam September 15th, 2009 | Author: Miami Urology Miami urology doctors are offering a free PSA Test, DRE exam (digital rectal exam)
http://www.nydailynews.com/lifestyle/health/2009/06/08/2009-06-08
_free_psa_prostate_screening_locations.html
Free PSA Prostate Screening Locations Monday, June 8th 2009, 2:43 PM
Prostate cancer is the second-most common type of cancer among men, affecting 1 in 6 American males (only skin cancer is more common). According to the Prostate Cancer Foundation, more than 192,000 Americans will be diagnosed with prostate cancer this year – that’s one new case occurs every 2.7 minutes. But for all of the astonishingly high numbers, prostate cancer is one of the most-treatable forms of the disease. In general, the earlier it is caught, the more likely it is for the patient to be cured and remain disease-free. Which makes screening so vital. The New York Daily news is offering all men aged 40 and over a FREE PSA prostate cancer test between Sunday, June 21 and Sunday, June 28, 2009. The simple blood test takes only minutes — yet it could save your life or the life of a loved one. Please see below for the location in your area.
http://www.abc15.com/content/living/yourhealth/story/
Free-screening-event-to-fight-deadly-cancer-in-men/vfA8Xj-mr0qgyJMbg3-thg.cspx
Free screening event to fight deadly cancer in men: Eva Bowen 9/23
Otis Brawley MD: PSA Screening leads to overdiagniosis, unneccessary treatment and saves relatively few lives. Free Screening Progams plays on our fears – Financial Incentives.
http://jnci.oxfordjournals.org/cgi/content/full/djp310
Journal of the National Cancer Institute Advance Access published online on August 31, 2009
Prostate Cancer Screening; Is This a Teachable Moment? Otis W. Brawley
Affiliations of author : American Cancer Society, Altanta, GA; Departments of Hematology and Oncology, Department of Medicine, and Department of Epidemiology, Emory University, Altanta, GA
Correspondence to: In this issue of the Journal, Welch and Albertsen (1) presented information that every man considering prostate cancer screening and treatment should know and understand. Prostate cancer screening has resulted in substantial overdiagnosis and in unnecessary treatment. It may have saved relatively few lives. Results from this article and recent results from prostate cancer screening and prevention trials demand reflection about what we as a society have done and are doing. Lessons to be learned have ethical and economic implications and involve our lack of respect for the scientific process and scientific evidence.
As I sat down to write this editorial, I heard a radio commercial that brings perspective to the issue. A local celebrity was promoting prostate cancer awareness. He said, “Prostate cancer is 100% curable when caught early.” He encouraged all men to get screened and announced that a van was touring the area offering screening in supermarket parking lots. This was a community service project sponsored by the radio station, the supermarket chain, and a radiation oncology practice.
A commercial like this plays to our fears and prejudices. All of us have been taught from an early age that the best way to deal with cancer is to find it early. With the development of the prostate-specific antigen test, prostate cancer screening and early detection efforts surged in the United States in the late 1980s and continue to this day (2,3). By 1991, there were large prostate cancer awareness campaigns, health systems, and others who stood to profit from prostate cancer screening and treatment and encouraged it, implying benefit to those screened (4). Many were eager to push screening because of a financial incentive; some simply did not think too deeply due to the financial gain. Others truly thought they were doing a public service and felt urgency because prostate cancer is a leading cause of cancer death.
Although there was clear evidence of early detection, there was little evidence to show that screening decreased prostate cancer mortality or saved lives. There was strong vocal “expert opinion” that surrogate endpoints of earlier stage at diagnosis and increased survival indicated that screening saved lives. Some experts expressed legitimate concern that screening was unproven and premature (5). Collins and Barry (6) noted that screening advocates were using the same mistaken arguments that caused the advocacy of lung cancer screening with chest X-ray in the 1960s. This intervention was abandoned in the 1970s after trials showed it ineffective.
Many screening advocates (both physician and lay) have had difficulty accepting that some cancers are not going to progress and cause symptoms or death within the lifetime of the patient (7). The distinguished urologist Willet Whitmore recognized overdiagnosis as a problem in his famous quote, “The quandary in prostate cancer: Is cure necessary in those for whom it is possible, and is cure possible in those for whom it is necessary?”(8)
Truth be known, most of our pathological definitions of cancer were developed in the mid-1800s using light microscopy (9). Prostate cancer has not moved fully into the molecular and genetic age (10). We desperately need the ability to predict which patient has a localized cancer that is going to metastasize and cause suffering and death and which patient has a cancer that is destined to stay in the patient’s prostate for the remainder of his life.
http://blog.lib.umn.edu/schwitz/healthnews/2009/08/powerful-editor.html
Problem with the PSA test. The problem with this test is that it tends to create fear and anxiety in many men with no real basis. Nobody knows beforehand which men probably will not need treatment and who will. But by the time that a man tests positive for a PSA, he may be in advanced stages of cancer when the probability of conventional treatment success is low. And if a man was not going to have any problems with cancer, is it really ethical to ask him to basically lose his manhood and dignity because of what basically amounts to a hunch?
The bottom line is that ED and incontinence are a very high price to pay for a test result of “maybe”. But it should be an informed, researched decision, not a decision where people are pressured, and frightened into undergoing treatment. A cancer diagnosis is extremely stressful, and many people will simply undergo treatment because of their fear of death, regardless of how small the probability of it may be.
http://www.drmcdougall.com/misc/2009nl/aug/king.htm
Larry King Live on Prostate Cancer Screening (PSA)- Show Sets a New Standard for Disease Mongering. Prostate cancer is being over-diagnosed and over-treated, and the current excessive use of PSA screening is unwarranted
Dr Thomas Stamey
http://www.ncbi.nlm.nih.gov/pubmed/15371827
J Urol. 2004 Oct;172(4 Pt 1):1297-301.
The prostate specific antigen era in the United States is over for prostate cancer: what happened in the last 20 years? Stamey TA, Caldwell M, McNeal JE, Nolley R, Hemenez M, Downs J. Department of Urology, School of Medicine, Stanford University, Stanford, California 94305,
PURPOSE: We assessed how well preoperative serum prostate specific antigen (PSA) reflects the largest cancer in consecutive untreated radical prostatectomies during the last 20 years at Stanford University.
MATERIALS AND METHODS: A total of 1,317 consecutive radical prostatectomies were divided into 4, 5-year periods between August 1983 and July 2003, and examined sequentially in 3 mm step sections by 1 pathologist. The largest cancer and 5 other histological variables in each prostate were measured. Preoperative clinical stages were tabulated for each 5-year period. Means, Pearson correlation coefficients, % change and multiple regression were used to compare selected variables.
RESULTS: Most parameters decreased linearly during the 20 years, including palpable nodules on digital rectal examination from 91% to 17%, mean age from 64 to 59 years, mean serum PSA from 25 to 8 ng/ml, and index (largest) cancer volume from 5.3 to 2.4 cc. Percent Gleason grade 4/5 of the largest cancer averaged 27% to 35% and prostate weight 44 to 53 gm. Contrasting August 1983 to December 1988 with January 1999 to July 2003, 6 histological cancer parameters had statistically significant relationships to serum PSA in the first period. In the last 5 years serum PSA was related only to prostate size.
CONCLUSIONS: Serum PSA was related to prostate cancer 20 years ago. In the last 5 years serum PSA has only been related to benign prostatic hyperplasia. There is an urgent need for serum markers that reflect the size and grade of this ubiquitous cancer.
http://latimesblogs.latimes.com/booster_shots/2008/08/psa-test-dont-d.html
PSA test: Don’t do it, say angry men August 4, 2008 | 2:00 pm
It adds up to many men receiving emasculating therapy when medical science cannot say definitively that they need it. The documentary screening, says Shapiro, was timed to counteract all the public service announcements seen on Father’s Day urging men to take the PSA test to be screened for prostate cancer.
The test gained FDA approval after Dr. Thomas Stamey published the first paper in 1987 in the New England Journal of Medicine claiming that it could be used to diagnose early prostate cancer. He’s come full circle, and no longer supports the test as a screening tool, saying “The PSA era is over in the United States.”
The debate isn’t over. American Medical Assn. says that PSA screening is unwarranted. Now the U.S. Preventive Services Task force says there’s not enough evidence to warrant doing it, and those over 75 should not have the test.
http://www.bmj.com/cgi/content/full/324/7332/255/a/DC1
Prostate debate. In the United States, questioning cancer screening is a risky business
Many people in America see health screening as a panacea. Screening, the thinking goes, wards off disease and allows people to stay healthy, perhaps forever. Those who question this fairytale view, as we have just discovered, are considered traitors, or even murderers.
On 18 December 2001, the San Francisco Chronicle published an article about Dusty Baker, manager of the Giants, the city’s baseball team. Baker had just had surgery for prostate cancer. His cancer, said the article, had been picked up after a routine blood test for prostate specific antigen (PSA).
http://www.bmj.com/cgi/eletters/324/7332/255/a/DC1#19194
Bertrand M.l Bell, Distinguished University Professor Albert Einstein College of medicine
the digital rectal examination and the prostate specific antigen are unreliable as tests to screen for prostate cancer. These tests are responsible for the epidemic of radical prostectomies in the US. Therapy for a histological finding of uncertain significance has not improved mortality from prostate cancer. What this surgery has done at least among the many men I have seen is to guarantee them incontinence and impotence!!
Free PSA- also see image
http://jama.ama-assn.org/cgi/content/abstract/279/19/1542
Use of the Percentage of Free Prostate-Specific Antigen to Enhance Differentiation of Prostate Cancer From Benign Prostatic Disease A Prospective Multicenter Clinical Trial
William J. Catalona, MD; Alan W. Partin, MD, PhD; Kevin M. Slawin, MD; Michael K. Brawer, MD; Robert C. Flanigan, MD; Anup Patel, MD; Jerome P. Richie, MD; Jean B. deKernion, MD; Patrick C. Walsh, MD; Peter T. Scardino, MD; Paul H. Lange, MD; Eric N. P. Subong, MS; Robert E. Parson, MS; Gail H. Gasior, BA; Kathleen G. Loveland, BS; Paula C. Southwick, PhD
JAMA. 1998;279:1542-1547.
Context.— The percentage of free prostate-specific antigen (PSA) in serum has been shown to enhance the specificity of PSA testing for prostate cancer detection, but earlier studies provided only preliminary cutoffs for clinical use.
Objective.— To develop risk assessment guidelines and a cutoff value for defining abnormal percentage of free PSA in a population of men to whom the test would be applied.
Design.— Prospective blinded study using the Tandem PSA and free PSA assays (Hybritech Inc, San Diego, Calif).
Setting.— Seven nationwide university medical centers.
Participants.— A total of 773 men (379 with prostate cancer, 394 with benign prostatic disease) 50 to 75 years of age with a palpably benign prostate gland, PSA level of 4.0 to 10.0 ng/mL, and histologically confirmed diagnosis.
Main Outcome Measures.— A percentage of free PSA cutoff that maintained 95% sensitivity for prostate cancer detection, and probability of cancer for individual patients.
Results.— The percentage of free PSA may be used in 2 ways: as a single cutoff (ie, perform a biopsy for all patients at or below a cutoff of 25% free PSA) or as an individual patient risk assessment (ie, base biopsy decisions on each patient’s risk of cancer). The 25% free PSA cutoff detected 95% of cancers while avoiding 20% of unnecessary biopsies. The cancers associated with greater than 25% free PSA were more prevalent in older patients, and generally were less threatening in terms of tumor grade and volume. For individual patients, a lower percentage of free PSA was associated with a higher risk of cancer (range, 8%-56%). In the multivariate model used, the percentage of free PSA was an independent predictor of prostate cancer (odds ratio [OR], 3.2; 95% confidence interval [CI], 2.5-4.1; P<.001) and contributed significantly more than age (OR, 1.2; 95% CI, 0.92-1.55) or total PSA level (OR, 1.0; 95% CI, 0.92-1.11) in this cohort of subjects with total PSA values between 4.0 and 10.0 ng/mL.
Conclusions.— Use of the percentage of free PSA can reduce unnecessary biopsies in patients undergoing evaluation for prostate cancer, with a minimal loss in sensitivity in detecting cancer. A cutoff of 25% or less free PSA is recommended for patients with PSA values between 4.0 and 10.0 ng/mL and a palpably benign gland, regardless of patient age or prostate size. To our knowledge, this study is the largest series to date evaluating the percentage of free PSA in a population representative of patients in whom the test would be used in clinical practice.
Stamey: PSA era is over.
Correlation of PSA with Prostte Cancer was good 20 years ago. This has changed.
http://www.innovations-report.com/html/reports/medicine_health/report-33457.html
The PSA era is over in the United States,” said Thomas Stamey, MD, professor of urology and lead author of the study published in the October issue of the Journal of Urology. “Our study raises a very serious question of whether a man should even use the PSA test for prostate cancer screening any more.”
The PSA test measures prostate specific antigen, a protein normally produced by the prostate gland. Stamey published the original findings in 1987 in the New England Journal of Medicine showing that increased blood PSA levels could be used to indicate prostate cancer. However, through the years, Stamey has come to believe that the PSA test is actually not a useful predictor of the amount or severity of prostate cancer. He said elevated levels of that protein actually reflect a condition called benign prostatic hyperplasia, a harmless increase in prostate size.
For the study, they used prostate tissue samples collected by professor John McNeal, MD, who has examined more than 1,300 prostates removed by different urologists at Stanford in the last 20 years. The researchers divided McNeal’s data into four five-year periods between 1983 and 2004 and looked at the characteristics of each cancer. They found that over time, there was a substantial decrease in the correlation between PSA levels and the amount of prostate cancer – from 43 percent predictive ability in the first five-year group down to 2 percent in the most recent one.
However, the Stanford researchers concluded that the PSA test is quite accurate at indicating the size of the prostate gland, meaning that it is a direct measure of benign prostatic hyperplasia. And Stamey pointed out that it is still very useful for monitoring patients following prostate removal as an indicator of residual prostate cancer that has spread to other parts of the body. “Our job now is to stop removing every man’s prostate who has prostate cancer,” said Stamey. “We originally thought we were doing the right thing, but we are now figuring out how we went wrong.
Rebuttal to Stamey by Catalona
http://www.europeanurology.com/article/S0302-2838(05)00449-5/fulltext
The PSA Era is not Over for Prostate Cancer- William J. Catalona * , Stacy Loeb.
Accepted 20 July 2005, pages 541 – 545 Acknowledgements -Dr. Catalona’s research is supported in part by Beckman Coulter Incorporated, a manufacturer of PSA tests.
Based on the currently available data, we believe that PSA screening should begin at age 40 when the PSA level should be well below 1 ng/ml and PSA testing should be repeated annually. Biopsy should be considered if the PSA is rising and does not return to baseline levels with antibiotic therapy or repeat measurements. PSA should be used intelligently, incorporating PSA derivatives such as PSA velocity, PSA density, percentage of free or percentage of complexed PSA, and, perhaps in the future, B-PSA and pro-PSA, in addition to the total PSA value.
Biopsy should be recommended if the PSA velocity exceeds 0.2 to 0.5 ng/ml/year in men with a total PSA level less than 2.5 ng/ml/year (more data is needed to determine optimal PSA velocity cutoffs, and perhaps a percentage change in the range of 20% per year will prove useful), or if the PSA velocity is greater than 0.75 ng/ml/year and the total PSA is above 4 ng/ml. Biopsy also should be considered if the total PSA is higher than 2.5 ng/ml and the PSA density is greater than 0.1 ng/ml/year or if the percentage of free PSA is less than 10%. These measures should help identify life-threatening prostate cancers at a stage when they can be cured.
Conservative Management of Prostate CA
http://www.ncbi.nlm.nih.gov/pubmed/19755699
JAMA. 2009 Sep 16;302(11):1202-9. Outcomes of localized prostate cancer following conservative management. Lu-Yao GL at al.
CONTEXT: Most newly diagnosed prostate cancers are clinically localized, and major treatment options include surgery, radiation, or conservative management. Although conservative management can be a reasonable choice, there is little contemporary prostate-specific antigen (PSA)-era data on outcomes with this approach. OBJECTIVE: To evaluate the outcomes of clinically localized prostate cancer managed without initial attempted curative therapy in the PSA era.
DESIGN, SETTING, AND PARTICIPANTS: A population-based cohort study of men aged 65 years or older when they were diagnosed (1992-2002) with stage T1 or T2 prostate cancer and whose cases were managed without surgery or radiation for 6 months after diagnosis. Living in areas covered by the Surveillance, Epidemiology, and End Results (SEER) program, the men were followed up for a median of 8.3 years (through December 31, 2007). Competing risk analyses were performed to assess outcomes.
MAIN OUTCOME MEASURES: Ten-year overall survival, cancer-specific survival, and major cancer related interventions.
RESULTS: Among men who were a median age of 78 years at cancer diagnosis, 10-year prostate cancer-specific mortality was 8.3% (95% confidence interval [CI], 4.2%-12.8%) for men with well-differentiated tumors; 9.1% (95% CI, 8.3%-10.1%) for those with moderately differentiated tumors, and 25.6% (95% CI, 23.7%-28.3%) for those with poorly differentiated tumors. The corresponding 10-year risks of dying of competing causes were 59.8% (95% CI, 53.2%-67.8%), 57.2% (95% CI, 52.6%-63.9%), and 56.5% (95% CI, 53.6%-58.8%), respectively. Ten-year disease-specific mortality for men aged 66 to 74 years diagnosed with moderately differentiated disease was 60% to 74% lower than earlier studies: 6% (95% CI, 4%-8%) in the contemporary PSA era (1992-2002) compared with results of previous studies (15%-23%) in earlier eras (1949-1992). Improved survival was also observed in poorly differentiated disease. The use of chemotherapy (1.6%) or major interventions for spinal cord compression (0.9%) was uncommon.
CONCLUSIONS: Results following conservative management of clinically localized prostate cancer diagnosed from 1992 through 2002 are better than outcomes among patients diagnosed in the 1970s and 1980s. This may be due, in part, to additional lead time, overdiagnosis related to PSA testing, grade migration, or advances in medical care.
No increase in mortality in convervatively Managed Low Grade cases
http://jama.ama-assn.org/cgi/content/full/293/17/2095
http://www.ncbi.nlm.nih.gov/pubmed/15870412
20-year outcomes following conservative management of clinically localized prostate cancer.
Albertsen PC, Hanley JA, Fine J.
CONTEXT: The appropriate therapy for men with clinically localized prostate cancer is uncertain. A recent study suggested an increasing prostate cancer mortality rate for men who are alive more than 15 years following diagnosis.
OBJECTIVE: To estimate 20-year survival based on a competing risk analysis of men who were diagnosed with clinically localized prostate cancer and treated with observation or androgen withdrawal therapy alone, stratified by age at diagnosis and histological findings.
DESIGN, SETTING, AND PATIENTS: A retrospective population-based cohort study using Connecticut Tumor Registry data supplemented by hospital record and histology review of 767 men aged 55 to 74 years with clinically localized prostate cancer diagnosed between January 1, 1971, and December 31, 1984. Patients were treated with either observation or immediate or delayed androgen withdrawal therapy, with a median observation of 24 years.
MAIN OUTCOME MEASURES: Probability of mortality from prostate cancer or other competing medical conditions, given a patient’s age at diagnosis and tumor grade.
RESULTS: The prostate cancer mortality rate was 33 per 1000 person-years during the first 15 years of follow-up (95% confidence interval [CI], 28-38) and 18 per 1000 person-years after 15 years of follow-up (95% CI, 10-29). The mortality rates for these 2 follow-up periods were not statistically different, after adjusting for differences in tumor histology (rate ratio, 1.1; 95% CI, 0.6-1.9). Men with low-grade prostate cancers have a minimal risk of dying from prostate cancer during 20 years of follow-up (Gleason score of 2-4, 6 deaths per 1000 person-years; 95% CI, 2-11). Men with high-grade prostate cancers have a high probability of dying from prostate cancer within 10 years of diagnosis (Gleason score of 8-10, 121 deaths per 1000 person-years; 95% CI, 90-156). Men with Gleason score of 5 or 6 tumors have an intermediate risk of prostate cancer death.
CONCLUSION: The annual mortality rate from prostate cancer appears to remain stable after 15 years from diagnosis, which does not support aggressive treatment for localized low-grade prostate cancer.
Both studies agree that men with well-differentiated tumors rarely die from their disease and that men with poorly differentiated tumors frequently die within 5 to 10 years of diagnosis, often despite aggressive interventions.
Men with low-grade prostate cancer have only a small risk of prostate cancer progression even after 20 years of management by observation or androgen withdrawal therapy alone. These results do not support aggressive treatment of localized low-grade prostate cancer. Men with poorly differentiated disease (Gleason scores of 7 and 8-10) have a high risk of death from prostate cancer; only 3 men were alive after 20 years. Men with moderate-grade disease (Gleason scores of 5-6) have an intermediate cumulative risk of prostate cancer progression after 20 years of follow-up.
http://jama.ama-assn.org/cgi/content/abstract/274/8/626
Long-term Survival Among Men With Conservatively Treated Localized Prostate Cancer
Peter C. Albertsen, MD; Dennis G. Fryback, PhD; Barry E. Storer, PhD; Thomas F. Kolon, MD; Judith Fine JAMA. 1995;274(8):626-631.
Results. —After a mean follow-up of 15.5 years, the age-adjusted survival for men with Gleason score 2 to 4 tumors was not significantly different from that of the general population. Maximum estimated lost life expectancy for men with Gleason score 5 to 7 tumors was 4 to 5 years and for men with Gleason score 8 to 10 tumors was 6 to 8 years. Tumor histologic findings and patient comorbidities were powerful independent predictors of survival.
Conclusions.—Compared with the general population, men aged 65 to 75 years with conservatively treated low-grade prostate cancer incur no loss of life expectancy. Men with higher-grade tumors (Gleason scores 5 to 10) experience a progressively increasing loss of life expectancy. Case series reports of survival/ mortality experienced by men with clinically localized prostate cancer that fail to control for age, tumor histologic features, and comorbidities risk significant bias.
http://jama.ama-assn.org/cgi/content/abstract/280/11/975
Competing Risk Analysis of Men Aged 55 to 74 Years at Diagnosis Managed Conservatively for Clinically Localized Prostate Cancer . Peter C. Albertsen, MD; James A. Hanley, PhD; Donald F. Gleason, MD, PhD; Michael J. Barry, MD JAMA. 1998;280:975-980.
Main Outcome Measures.— Estimates of the probability of dying from prostate cancer or other competing hazards.
Results.— Men with tumors that have Gleason scores of 2 to 4, 5, 6, 7, and 8 to 10 face a 4% to 7%, 6% to 11%, 18% to 30%, 42% to 70%, and 60% to 87% chance, respectively, of dying from prostate cancer within 15 years of diagnosis depending on their age at diagnosis.
Conclusions.— Men whose prostate biopsy specimens show Gleason score 2 to 4 disease face a minimal risk of death from prostate cancer within 15 years of diagnosis. Conversely, men whose biopsy specimens show Gleason score 7 to 10 disease face a high risk of death from prostate cancer when treated conservatively, even when cancer is diagnosed as late as age 74 years. Men with Gleason score 5 or 6 tumors face a modest risk of death from prostate cancer that increases slowly over at least 15 years of follow-up.
Histologic Grading of Prostate Cancer
http://www.ncbi.nlm.nih.gov/pubmed/12604893
Am J Surg Pathol. 2003 Mar;27(3):365-71.
Basal cell cocktail (34betaE12 + p63) improves the detection of prostate basal cells.
Zhou M, Shah R, Shen R, Rubin MA. Department of Pathology, University of Michigan School of Medicine, Ann Arbor, MI, USA.
http://www.ncbi.nlm.nih.gov/pubmed/15487448
Am J Clin Pathol. 2004 Oct;122(4):517-23. Usefulness of basal cell cocktail (34betaE12 + p63) in the diagnosis of atypical prostate glandular proliferations.
Shah RB, Kunju LP, Shen R, LeBlanc M, Zhou M, Rubin MA.
Gleason Grading
http://www.phoenix5.org/Infolink/GleasonGrading.html
Understanding Gleason Grading Last Revised May 14, 1997
http://www.prostate-cancer.org/education/staging/Dowd_GleasonScore.html
The Gleason Score: A Significant Biologic Manifestation of Prostate Cancer Aggressiveness On Biopsy By Gerry J. O’Dowd, Robert W. Veltri, M. Craig Miller, UroCor, Inc., Oklahoma City, OK;
and Stephen B. Strum, Prostate Cancer Research Institute, Los Angeles, CA
Reprinted from PCRI Insights January 2001 v4.1
http://www.yananow.net/Chart-Gleason.htm
YANA – YOU ARE NOT ALONE NOW – PROSTATE CANCER SUPPORT SITE
TREATMENT CHOICES INDEXED BY – GLEASON SCORE AT DIAGNOSIS
Active Surveillance of Prostate
http://jco.ascopubs.org/cgi/content/abstract/23/32/8165
Journal of Clinical Oncology, Vol 23, No 32 (November 10), 2005: pp. 8165-8169
Active Surveillance for Prostate Cancer: For Whom? Laurence Klotz
Prostate-specific antigen (PSA) –based prostate cancer screening results in the diagnosis of prostate cancer in many men who are not destined to have clinical progression during their lifetime. Good-risk prostate cancer, defined as a Gleason score of 6 or less, PSA < 10, and T1c to T2a, now constitutes 50% of newly diagnosed prostate cancer. In most of these patients, the disease is indolent and slow growing. The challenge is to identify those patients who are unlikely to experience significant progression while offering radical therapy to those who are at risk. The approach to favorable-risk prostate cancer described in this article uses estimation of PSA doubling time (PSA DT) to stratify patients according to the risk of progression. Patients who select this approach are managed initially with active surveillance. Those who have a PSA DT of 3 years or less (based on a minimum of three determinations over 6 months) are offered radical intervention. The remainder are closely monitored with serial PSA and periodic prostate rebiopsies (at 2, 5, and 10 years). In this series of 299 patients, the median DT was 7 years. Forty-two percent had a PSA DT > 10 years, and 20% had a PSA DT > 100 years. The majority of patients on this study remain under surveillance. The approach of active surveillance with selective delayed intervention based on PSA DT represents a practical compromise between radical therapy for all (which results in overtreatment for patients with indolent disease) and watchful waiting with palliative therapy only (which results in undertreatment for those with aggressive disease).
http://www.pcngcincinnati.org/index.html
http://www.pcngcincinnati.org/psa/calculator.html
PSADT & PSAV Calculator
http://www.prostatecancerwatchfulwaiting.co.za/ActiveSurveillance.pdf
Actuve surveillance: towards a new paradigm in the management of early prostate cancer
Chris Parker
http://deb.uthscsa.edu/URORiskCalc/Pages/uroriskcalc.jsp
The Cancer Risk Calculator for Prostate Cancer was developed based upon 5519 men in the placebo group of the Prostate Cancer Prevention Trial. All of these 5519 men initially had a PSA value less than or equal to 3.0 ng/ml and were followed for seven years with annual PSA and digital rectal examination. If PSA exceeded 4.0 ng/ml or if an abnormal digital rectal examination was noted, a biopsy was recommended. After seven years, all men were recommended to have a prostate biopsy, regardless of PSA or rectal examination findings. PSA, family history, rectal examination findings, and history of a prior negative prostate biopsy provided independent predictive value to the calculation of risk of a biopsy that showed presence of cancer.
http://caonline.amcancersoc.org/cgi/content/full/56/2/106?
ijkey=59ae75ff6fdc610962e71f2b9d9bf29472a73127
Cancer Statistics, 2006 Ahmedin Jemal, DVM, PhD, Rebecca Siegel, MPH, Elizabeth Ward, PhD, Taylor Murray, Jiaquan Xu, Carol Smigal, MPH and Michael J. Thun, MD, MS
Prostate and female breast cancer incidence rates have continued to increase, although at a slower rate than in previous years. The continuing increase may be attributable to increased screening through prostate-specific antigen (PSA) testing for prostate cancer and mammography for breast cancer.
2007: Kvåle Rune; Auvinen Anssi; Adami Hans-Olov; Klint Asa; Hernes Eivor; Møller Bjørn; Pukkala Eero; Storm Hans H; Tryggvadottir Laufey; Tretli Steinar; Wahlqvist Rolf; Weiderpass Elisabete; Bray Freddie
Interpreting trends in prostate cancer incidence and mortality in the five Nordic countries.
Journal of the National Cancer Institute 2007;99(24):1881-7.
Trends in incidence and mortality rates of prostate cancer were analyzed using data from the national cancer registries of Denmark, Finland, Iceland, Norway, and Sweden. Joinpoint regression models were used to quantify temporal trends for the period from 1980 to 2004. Incidence rates were increasing and similar in the Nordic countries during the 1980s. Around 1990, a more rapid incidence increase began in all Nordic countries except Denmark, where an increase was seen 5 years later. In 2001, incidence rates in Denmark were half of those seen in the other Nordic countries, but mortality rates varied only marginally among countries. Mean annual declines in prostate cancer mortality of 1.9% (95% CI = 0.4% to 3.3%) and 1.8% (95% CI = 0.5% to 3.0%) were observed from 1996 to 2004 in Finland and Norway, respectively. During the same period, mortality rates leveled off in Iceland and Sweden but continued to increase in Denmark. The rapid increase in incidence during the early 1990s coincided with the introduction of the prostate-specific antigen (PSA) test and conveys little information about the occurrence of potentially lethal disease.
Mortality rates, however, have recently stabilized or declined in countries where PSA testing and curative treatment have been commonly practiced since the late 1980s. Although other explanatory factors may be in operation, these trends are consistent with a moderate effect of increased curative treatment of early diagnosed prostate cancer and improved treatment of more advanced disease.
http://jjco.oxfordjournals.org/cgi/content/abstract/39/6/339
Japanese Journal of Clinical Oncology Advance Access originally published online on April 4, 2009 Japanese Journal of Clinical Oncology 2009 39(6):339-351; doi:10.1093/jjco/hyp025
The Japanese Guideline for Prostate Cancer Screening
Chisato Hamashima1, Tomio Nakayama2, Motoyasu Sagawa3, Hiroshi Saito1 and Tomotaka Sobue4
In 2005, there were 9264 deaths from prostate cancer, accounting for 4.7% of the total number of cancer deaths in Japan. 1186 articles published from January 1985 to October 2006 were selected using MEDLINE and other methods.
After the systematic literature review, 28 articles were identified as providing evidence of mortality reduction from prostate cancer, including 5 observational studies for DRE screening, 1 meta-analysis, 3 randomized controlled trials and 19 observational studies for PSA screening. Although several studies showed that PSA screening had a beneficial effect, the results of the selected studies were inconsistent.
Overall, the evidence that screening reduced mortality from prostate cancer was insufficient. Furthermore, prostate cancer screening is associated with serious harms, including overdiagnosis, adverse effects of needle biopsy and adverse effects of local prostatectomy. At present, the evidence for the effect of prostate cancer screening is insufficient. Both PSA and DRE were not recommended for population-based screening programs, but they could be conducted as individual-based screening if basic requirements were met.
http://theoncologist.alphamedpress.org/cgi/content/full/13/3/306
The Oncologist, Vol. 13, No. 3, 306-308, March 2008; doi:10.1634/theoncologist.2008-0008
Commentary: How Serious Is Getting a Diagnosis of Prostate Cancer?
Michael J. Barry Medical Practices Evaluation Center, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts, USA
Correspondence: Michael J. Barry, M.D., General Medicine Unit, Massachusetts General Hospital, 50 Staniford Street—9th Floor, Boston, Massachusetts Received January 14, 2008; accepted for publication January 28, 2008.
http://www.phac-aspc.gc.ca/publicat/cdic-mcc/16-1sup/c_e.html
Trends in Incidence and Mortality of Prostate Cancer in Canada . Isra Levy
http://jnci.oxfordjournals.org/cgi/content/full/99/24/1881
BRIEF COMMUNICATION Interpreting Trends in Prostate Cancer Incidence and Mortality in the Five Nordic Countries . We conclude that the incidence rates of prostate cancer are closely related to the introduction of the PSA test. The recent stabilization or declines in prostate cancer mortality rates observed in four of the five Nordic countries are consistent with a modest effect of increased curative treatment of early diagnosed prostate cancer and improved treatment of more advanced disease.
Public Health Rep. 2004 Mar–Apr; 119(2): 174–186. PMCID: PMC1497609
Prostate cancer incidence and mortality rates and trends in the United States and Canada.
Kathleen McDavid, Judy Lee, John P Fulton, Jon Tonita, and Trevor D Thompson
OBJECTIVE: The purpose of this study was to compare prostate cancer incidence and mortality trends between the United States and Canada over a period of approximately 30 years.
METHODS: Prostate cancer incident cases were chosen from the National Cancer Institute’s Surveillance Epidemiology and End Results (SEER) Program to estimate rates for the United States white males and from the Canadian Cancer Registry for Canadian men. National vital statistics data were used for prostate cancer mortality rates for both countries, and age-adjusted and age-specific incidence and mortality rates were calculated. Joinpoint analysis was used to identify significant changes in trends over time.
RESULTS: Canada and the U.S. experienced 3.0% and 2.5% growth in age-adjusted incidence from 1969-90 and 1973-85, respectively. U.S. rates accelerated in the mid- to late 1980s. Similar patterns occurred in Canada with a one-year lag. Annual age-adjusted mortality rates in Canada were increasing 1.4% per year from 1977-93 then fell 2.7% per year from 1993-99. In the U.S., annual age-adjusted mortality rates for white males increased 0.7% from 1969-1987 and 3.0% from 1987-91, then decreased 1.2% and 4.5% during the 1991-94 and 1994-99 periods, respectively. CONCLUSIONS: Recent incidence patterns observed between the U.S. and Canada suggest a strong relationship to prostate-specific antigen (PSA) test use. Clinical trials are required to determine any effects of PSA test use on prostate cancer and overall mortality.
http://jnci.oxfordjournals.org/cgi/content/full/91/12/1017
Journal of the National Cancer Institute, Vol. 91, No. 12, 1017-1024, June 16, 1999
© 1999 Oxford University Press
Cancer Surveillance Series: Interpreting Trends in Prostate Cancer—Part I: Evidence of the Effects of Screening in Recent Prostate Cancer Incidence, Mortality, and Survival Rates
Benjamin F. Hankey, Eric J. Feuer, Limin X. Clegg, Richard B. Hayes, Julie M. Legler, Phillip C. Prorok, Lynn A. Ries, Ray M. Merrill, Richard S. Kaplan
Finally, in the analysis of the recent decrease in prostate cancer mortality, the antecedent acceleration in the trend merits some attention (Fig. 1). If this observation is an artifact associated with the rising and falling pool of newly diagnosed cases (e.g., a certain proportion of the pool could have a misclassified cause of death), then it would have implications for establishing the importance of the recent mortality decrease. It may be that the rates are returning to some background trend after having been perturbed by such an artifact. This possibility is explored in detail in the second paper in this series by Feuer et al. (18), which concludes that misclassification of cause of death is contributing to some extent to the increase and subsequent decline in prostate cancer mortality.
http://jnci.oxfordjournals.org/cgi/content/full/91/12/1025
Journal of the National Cancer Institute, Vol. 91, No. 12, 1025-1032, June 16, 1999
© 1999 Oxford University Press
Cancer Surveillance Series: Interpreting Trends in Prostate Cancer—Part II: Cause of Death Misclassification and the Recent Rise and Fall in Prostate Cancer Mortality
Eric J. Feuer, Ray M. Merrill, Benjamin F. Hankey
The trends in IBM shown in Figs. 3 and 5 probably represent the effect of many possible forces (screening, treatment, iatrogenic deaths, and attribution bias), many of which work in opposite directions. The fact that IBM rose above its background trend starting in the PSA era suggests that a factor such as attribution bias was more than offsetting any potential early benefits in prostate cancer mortality rates resulting from early detection or treatment. A continued decline in mortality to a level below the prescreening level would provide stronger evidence of an effect of screening. However, the fact that, until now, mortality has risen and fallen back to its prescreening level suggests that the recent trends may have been affected by cause-of-death misclassification associated with the rising and falling pool of prevalent cases.
http://www.eradimaging.com/site/article.cfm?ID=1
Prostate-Specific Antigen Test: Is It a Valid Screening Tool for Prostate Cancer?
Pamela C. Cartright, MAEd, RT(R)(T)
The current recommendation from the American Cancer Society and the American Urologic Association is that all men age 50 years and older should have yearly PSA and DRE screening, and that African American men and those with a family history of prostate cancer should begin screening at age 45 years.5,12 Conversely, the American Society of Internal Medicine, the American College of Physicians, and the US Preventative Services Task Force all recommend against routine screening.2
http://www.renegadeneurologist.com/prostate-treatment-wasted-40-billion-scientist-says/
Prostate Treatment Wasted $40 Billion, Scientist Says
From Bloomberg.com: Prostate-cancer therapies for men who didn’t need treatment cost at least $40 billion during two decades in the U.S., according to a Dartmouth Medical School researcher.
Kirsten Howard from the University of Sydney’s School of Public Health
http://www.usyd.edu.au/news/84.html?newsstoryid=3911
Testing not a major factor in prostate cancer mortality. 29 September 2009
Death from prostate cancer does not vary greatly between men who undergo annual prostate-specific antigen (PSA) screening and those who do not, according to an investigation of PSA outcomes.
“A Model of Prostate-Specific Antigen Screening Outcomes for Low- to High-Risk Men” was published in the Archives on Internal Medicine today. Dr Kirsten Howard from the University of Sydney’s School of Public Health was the paper’s lead author.
The paper compares diagnosis and mortality outcomes of men who undergo annual PSA tests with those who did not take the tests.
“Unsurprisingly, we found men who test for prostate cancer had a higher rate of diagnosis,” says Dr Howard. “But mortality rates from prostate cancer don’t decrease significantly for this group.
“Older men, and those whose close family members had the disease, experience a slightly lower mortality rate from prostate cancer if they take regular tests. But the difference among those aged between 40 and 50 or who are at low risk is statistically insignificant.”
Dr Howard says the high rate of diagnosis, when measured against the relatively low mortality rates, indicates men with PSA-detected cancer may often undergo therapies for clinically insignificant cancers.
“This is no small thing when you consider some of the side effects of further testing and treatment. Biopsies can cause haemorrhaging and infections while treatment carries with it the risk of impotence and/or incontinence.
The most striking finding from the model was that the absolute mortality benefit from regular screening was small even among men at the highest levels of risk “and even when prostate cancer deaths are cumulated to 85 years of age. This reflects the relatively small proportion of overall deaths due to prostate cancer and the fact that deaths from other causes partly offset those averted by screening,” Dr. Howard and her colleagues said (Arch. Intern. Med. 2009;169;1603-10).
The model also “provides a sobering illustration of the frequency of harms men are likely to experience if they participate in PSA screening.” As many as 21% of low-risk men will get a false-positive result during 10 years of annual screening, as will an even greater percentage of older men and men at higher risk.
Regular screening improved the odds of detecting prostate cancer by two- to fourfold, compared with no screening. However, few of the men in whom cancer is detected would die from it. Moreover, death rates from prostate cancer and from all causes were similar between men who underwent annual screening and men who had no screening.
“The only interpretation is that many men with screen-detected prostate cancer are having cancer therapies for clinicially insignificant cancers,” the investigators said.
This study was limited in that it evaluated mortality but not another outcome that many men would consider crucial: quality of life. Up to 70% of men treated for prostate cancer experience erectile dysfunction or impotence, up to 50% experience lifelong urinary incontinence, and up to 25% experience bowel problems, Dr. Howard and her associates said. Also, researchers relied on multiple sources for to estimate screening outcomes because there is no single organized screening program in Australia. They note specifically that “by assuming that every positive PSA screening result is investigated by means of biopsy, we may have overestimated the number of biopsies.” Further, they wrote, there were no data available, investigators were left to model the incidence of unscreened men.
In an editorial comment accompanying this report, Dr. Michael Pignone of the University of North Carolina in Chapel Hill concurred. The results of previous studies have suggested that “most men would not find screening to have net benefit if all relevant outcomes were considered.”
Taken together with the findings of other studies, this model provides “greater confidence that the risk reduction from screening is at best modest,” he said (Arch. Intern. Med. 2009;169:1554-6).
To date, no study has been able to “define the ‘correct’ trade-off between the more common and immediate downsides of overdiagnosis and treatment complications and the less common and deferred benefits of reduced risk of prostate cancer-related mortality. [However,] the work by Howard and colleagues is an important step in providing information to patients and providers to facilitate discussion about this trade-off.”
The work was funded by the National Health and Medical Research Council of Australia. Neither Dr. Howard nor Dr. Pignone reported any financial conflicts of interest.
http://archinte.ama-assn.org/cgi/content/full/169/17/1554?home
Weighing the Benefits and Downsides of Prostate-Specific Antigen Screening
Pignone Arch Intern Med.2009; 169: 1554-1556.
http://health.usnews.com/articles/health/healthday/
2009/09/28/men-not-being-told-enough-about-psa-tests.html
Men Not Being Told Enough About PSA Tests Pros, cons of cancer screen not understood, research shows Posted September 28, 2009
Otis Brawley MD
http://www.medicalnewstoday.com/articles/143145.php
http://www.patientadvocate.org/index.php?p=458
http://www.cancer.org/docroot/MED/content/
MED_2_1x_American_Cancer_Society_Names_New_Chief_Medical_Officer.asp
Otis W. Brawley is professor of hematology, oncology, and medicine at the Emory University School of Medicine and Professor of Epidemiology at the Emory Rollins School of Public Health. He also serves as associate director of the Winship Cancer Institute at Emory University. In addition Dr. Brawley is chief of hematology and oncology services and the medical director of the Georgia Cancer Coalition Center of Excellence at Grady Memorial Hospital.
From 1995 to April 2001, he served as Assistant Director of the Office of Special Populations Research at the National Cancer Institute. Dr. Brawley was previously a senior in the Division of Cancer Prevention and Control at the National Cancer Institute where he was one of a group instrumental in the development and launching of the Prostate Cancer Prevention Trial. This 18,000-man trial is looking at screening and epidemiologic issues in prostate cancer as well as the potential for prevention of benign prostatic hyperplasia and prostate cancer. He also served as Chief of the NCI Intramural Prostate Cancer Clinic from 1993–1995.
Otis W. Brawley, MD, Chief Medical Officer of the American Cancer Society (ACS), has been selected as the 2009 J. Rhodes Haverty Lecture speaker. American Cancer Society Names New Chief Medical Officer Otis Webb Brawley, M.D. to Succeed Harmon J. Eyre, M.D Atlanta 2007/07/23
Interview with Otis Brawley:
About Prosate Cancer screning with PSA test: we still cannot say whether the benefits outweigh the risk.
About 2009 PSA screening studies: Now as these reports have begun to come out, we see that the results may not be as favorable as many had hoped or even anticipated.
PSA still useful as part of diagnostic workup for symptoms:There is no debate that men who have urinary symptoms, such as frequent or difficult urination, a weak stream, etc., ought to be getting exams including PSA tests. That is not screening; screening is testing asymptomatic men for signs of cancer. Men who have symptoms should be getting tests.
Amer Cancer Society opposed to screening:In fact, a discussion in this same issue of the New England Journal of Medicine misportrays the American Cancer Society guideline, saying the Society recommends screening. We do not recommend screening for men at average risk; we recommend shared decision making.
http://www.psa-rising.com/upfront/otisbrawleyfeb00.htm
Otis Brawley: I have never had a PSA and do not desire one. I have had relatives with the disease. I just do not believe it saves that many lives.
I did attend a series of meetings in 1997 when the ACS gathered fifty leading cancer specialists (epidemiologists and treaters) to re-evaluate their screening recommendation. This meeting led to the ACS repealing their recommendation that all men over fifty get screened and instituting a recommendation that men be offered the test and informed of potential risks and benefits. This latter recommendation was adopted in June 1997.
It is unfortunate that you have interpreted my writings as against screening. Indeed if you carefully review them, I am against misleading people by saying it clearly saves lives and there are minimal downsides.
I should note that I am aware of twenty three different organizations of experts in screening around the world who have considered the question and all have chosen not to make the blanket statement that screening saves lives and men should be screened. Most actually recommend men not get the test because it is not proven effective.
My point is that when twenty-three organizations of experts from the Canadian Urology Association to the American College of Physicians to the U.S. Preventive Services Task Force recommend against screening and men are encouraged to get and not told that the predominance of professional expert opinion is that it is unproven and should not be done then they are being misled and misinformed
Indeed there are now several studies that suggest that perhaps a third of all men diagnosed by PSA and quote “cured” would never have been bothered by their disease without our current screening technologies. They would have lived long not knowing they had prostate cancer and ultimately died of something unrelated.
There is also the issue that nearly 40% of men diagnosed and “cured” with radical prostatectomy ultimately relapse with metastatic prostate cancer. For most of these men early detection (no matter how early) would not save their lives.
In reality I know private industry benefits from prostate cancer screening, I do not know that the men who are screened benefit.
http://caonline.amcancersoc.org/cgi/content/full/59/4/225
Cancer Statistics, 2009
Ahmedin Jemal, DVM, PhD1, Rebecca Siegel, MPH2, Elizabeth Ward, PhD3, Yongping Hao, PhD4, Jiaquan Xu, MD5 and Michael J. Thun, MD, MS6
Published online before print May 27, 2009
CA Cancer J Clin 2009; 59:225-249
http://caonline.amcancersoc.org/content/vol59/issue4/images/large/CAAC20006fig003.jpeg
FIGURE 3 Annual Age-adjusted Cancer Incidence Rates among Males and Females for Selected Cancers, United States, 1975– 2005.
Rates are age adjusted to the 2000 US standard population and adjusted for delays in reporting. Source: Surveillance, Epidemiology, and End Results (SEER) program (www.seer.cancer.gov). Delay-adjusted incidence database, SEER Incidence Delay-Adjusted Rates, from nine registries, 1975 to 2005. National Cancer Institute, DCCPS, Surveillance Research Program, Statistical Research and Applications Branch, released April 2008, based on the November 2007 SEER data submission.
http://caonline.amcancersoc.org/content/vol59/issue4/images/large/CAAC20006fig004.jpeg
FIGURE 4 Annual Age-adjusted Cancer Death Rates among Males for Selected Cancers, United States, 1930–2005.
Rates are age adjusted to the 2000 US population. Due to changes in ICD coding, numerator information has changed over time. Rates for cancers of the lung and bronchus, colon and rectum, and liver are affected by these changes. Source: US mortality data, 1960 to 2005, US Mortality Vol. 1930–1959, National Cancer Institute, Centers for Disease Control and Prevention, 2008.
Screening Guidlelines
http://www.psa-rising.com/mednews/component/content/article/38-screening/78-aua-new-guidelines-on-prca-screening
Screening for prostate cancer
AUA New Guidelines on Prostate Cancer Screening Tuesday, April 28 2009 01:21
AUA advises that the prostate-specific antigen (PSA) test should be offered to well-informed men aged 40 years or older who have a life expectancy of at least 10 years.
AUA’s statement on the guidelines continues: “The PSA test, as well as how it is used to guide patient care (e.g., at what age men should begin regular testing, intervals at which the test should be repeated, at what point a biopsy is necessary) is highly controversial; however, the AUA believes that when offered and interpreted appropriately. the PSA test may provide essential information for the diagnosis, pre-treatment staging or risk assessment and post-treatment monitoring of prostate cancer.”
http://www.webmd.com/prostate-cancer/news/20090427/psa-screening-guidelines-stir-debate
PSA Screening Guidelines Stir Debate. American Urological Association Calls for PSA Screening at Age 40 to Help Detect Prostate Cancer By Salynn Boyles WebMD Health NewsReviewed by Louise Chang, MDApril 27, 2009 — A new recommendation that men consider prostate-specific antigen (PSA) testing a decade earlier than is now the norm is being widely criticized by some of the nation’s top prostate cancer experts
active surveillance
http://www.ncbi.nlm.nih.gov/pubmed/16414494
Active surveillance with selective delayed intervention for favorable risk prostate cancer.
Klotz L. Division of Urology, University of Toronto,
Good risk prostate cancer, defined as a Gleason score of < or = 6, prostate-specific antigen (PSA) <10, and T1c-T2a, now constitutes 50% of newly diagnosed prostate cancer. Recent data from the Prostate Cancer Prevention Trial, Stamey data set on PSA-prostate cancer correlations, and the Surveillance, Epidemiology, and End Results database make it very clear that a policy of PSA screening with biopsy for those patients in whom PSA is increased results in the diagnosis, and radical treatment, of a very large proportion of men who do not have life-threatening prostate cancer. Most men with good risk prostate cancer have indolent and slow growing disease. The challenge is to identify those patients who are unlikely to have significant progression, while offering radical therapy to those who are at risk. The approach to favorable risk prostate cancer described in this article uses estimation of PSA doubling time (DT) and repeat biopsy to stratify patients according to the risk of progression. Patients who select this approach are treated initially with active surveillance. Those patients who have a PSA DT of < or = 3 years (based on a minimum of 3 determinations over 6 months) are offered radical intervention. The remaining patients are closely monitored with serial PSA and periodic prostate repeat biopsy at 1, 4, 7, and 10 years. In one series of 299 patients treated in this way, 65% remained free of treatment at 8 years. The prostate cancer specific survival using this approach was 99.3% at 8 years. The majority of patients in this study remain on surveillance. Active surveillance with selective delayed intervention based on PSA DT is a practical middle ground between radical therapy for all, which results in over-treatment of patients with indolent disease, and watchful waiting with palliative therapy only, which results in under-treatment of those with aggressive disease.
http://www.europeanurology.com/article/S0302-2838(07)00713-0/pdf Prospective Validation of Active Surveillance in Prostate Cancer: The PRIAS Study RCN van den Bergh, S Roemeling, MJ Roobol … – europeanurology.com
European Urology, Volume 52, Issue 6, Pages 1560-1563, December 2007, Authors:Roderick CN van den Bergh; Stijn Roemeling; Monique J. Roobol; Wouter Roobol; Fritz H. Schröder; Chris H. Bangma.
http://www.prostatecancerwatchfulwaiting.co.za/HardieParker2005.pdf
Early outcomes of active surveillance for localized prostate cancer C Hardie, C Parker, A Norman, R Eeles, A … – BJU international, 2005
http://www3.interscience.wiley.com/journal/113385414/abstract
PSA doubling time predicts the outcome after active surveillance in screening-detected prostate cancer: Results from the European randomized study of screening for prostate cancer, Sweden section Khatami Ali 1 *, Aus Gunnar 1, Damber Jan-Erik 1, Lilja Hans 2 3, Lodding Pär 1, Hugosson Jonas 1 Sweden
http://www3.interscience.wiley.com/cgi-bin/fulltext/118859241/HTMLSTART
Cancer. 2008 Jun 15;112(12):2664-70
Active surveillance for the management of prostate cancer in a contemporary cohort.
Dall’Era MA, Konety BR, Cowan JE, Shinohara K, Stauf F, Cooperberg MR, Meng MV, Kane CJ, Perez N, Master VA, Carroll PR.
Department of Urology and the Helen Diller Family Comprehensive Cancer Center, University of California at San Francisco,
BACKGROUND: Active surveillance followed by selective treatment for men who have evidence of disease progression may be an option for select patients with early-stage prostate cancer. In this article, the authors report their experience in a contemporary cohort of men with prostate cancer who were managed with active surveillance.
METHODS: All men who were managed initially with active surveillance were identified through the authors’ institutional database. Selection criteria for active surveillance included: prostate-specific antigen (PSA)<10 ng/mL, biopsy Gleason sum </=6 with no pattern 4 or 5, cancer involvement of <33% of biopsy cores, and clinical stage T1/T2a tumor. Patients were followed with PSA measurements and digital rectal examination every 3 to 6 months and with transrectal ultrasound at 6- to 12-month intervals. Beginning in 2003, patients also underwent repeat prostate biopsy at 12 to 24 months. The primary outcome measured was active treatment. Evidence of disease progression, defined as an increase in rebiopsy Gleason sum or significant PSA velocity changes (>0.75 ng/mL per year), was a secondary outcome. Chi-square and log-rank tests were used to compare groups. The association between clinical characteristics and receipt of active treatment was analyzed by using Cox proportional hazards regression.
RESULTS: Three hundred twenty-one men (mean age [+/-standard deviation]: 63.4+/-8.5 years) selected active surveillance as their initial management. The overall median follow-up was 3.6 years (range, 1-17 years). The initial mean PSA level was 6.5+/-3.9 ng/mL. One hundred twenty men (37%) met at least 1 criterion for progression. Overall, 38% of men had higher grade on repeat biopsy, and 26% of men had a PSA velocity>0.75 ng/mL per year. Seventy-eight men (24%) received secondary treatment at a median 3 years (range, 1-17 years) after diagnosis. Approximately 13% of patients with no disease progression elected to obtain treatment. PSA density at diagnosis and rise in Gleason score on repeat biopsy were associated significantly with receipt of secondary treatment. The disease-specific survival rate was 100%.
CONCLUSIONS: Selected individuals with early-stage prostate cancer may be candidates for active surveillance. Specific criteria can be and need to be developed to select the most appropriate individuals for this form of management and to monitor disease progression. A small attrition rate can be expected because of men who are unable or unwilling to tolerate surveillance. Copyright (c) 2008 American Cancer Society.
Although there is increasing interest in examining active surveillance as a legitimate management approach for low-risk prostate cancer, the criteria for patient selection and definition of progressive disease vary between studies.[8-10][18] In general, most active surveillance studies have restricted patient selection by using Gleason grade and PSA cutoff points; however, specific threshold values vary between studies. Klotz entered patients with Gleason scores 7, whereas we restricted the candidates to those with Gleason scores 6.[19] Carter et al. used PSA values 20 ng/mL, whereas our cohort generally was limited to men who had PSA values <10 ng/mL.[8] The inclusion of patients with higher Gleason scores and higher PSA values likely groups patients with pure low-risk features and those with intermediate risk features together and may affect progression estimates and treatment outcomes.
Although disease progression determined by PSA or Gleason grade is observed in approximately 33% of these low-risk patients, secondary treatment is adopted by only a subset of these patients, and the others remain on active surveillance. Gleason grade change is the most important driver for the initiation of secondary treatment in our experience.
http://www.ncbi.nlm.nih.gov/pubmed/17850361
BJU Int. 2008 Jan;101(2):165-9. Epub 2007 Sep 10.
Active surveillance; a reasonable management alternative for patients with prostate cancer: the Miami experience.
Soloway MS, Soloway CT, Williams S, Ayyathurai R, Kava B, Manoharan M.
Department of Urology, University of Miami Miller School of Medicine, Miami, Florida 33101, USA.
OBJECTIVE: To examine the outcome of patients diagnosed with ‘low-risk’ prostate cancer managed by active surveillance (AS). PATIENTS AND METHODS: In all, 157 men with localized prostate cancer were followed on AS. The inclusion criteria for AS included: Gleason score of < or = 6, a serum prostate-specific antigen (PSA) level of < or = 15 ng/mL, stage < or = T2, low-volume disease and > 12 months of follow-up. The follow-up was rigorous, with PSA tests and a digital rectal examination every 3 months for 2 years, and a repeat biopsy 6-12 months after the initial diagnosis and yearly when indicated. Continuance of AS was based on the PSA doubling time, re-biopsy score, Gleason score, tumour volume, stage progression and patient preference.
RESULTS: In all 99 patients met the inclusion criteria; their mean age at diagnosis was 66 years, their mean PSA level 5.77 ng/mL and the mean follow-up 45.3 months. On initial repeat biopsy, 63% had no cancer and 34% had a Gleason sum of < or = 6. Eight patients were treated (three with hormones; five with curative intent); two had radical prostatectomy (one had pT2c pNO Gleason 7 disease); three had radiotherapy. The probability is that 85% would remain treatment-free at 5 years; no patient died from prostate cancer. The PSA doubling time and clinical stage at diagnosis were predictive of progression. CONCLUSION: Patients who are followed on AS must be selected using narrowly defined inclusion criteria and closely followed with a standard regimen of PSA testing, digital rectal examination and repeat biopsy.
http://www.ncbi.nlm.nih.gov/pubmed/19233410
J Urol. 2009 Apr;181(4):1635-41;
A multi-institutional evaluation of active surveillance for low risk prostate cancer.
Eggener SE, Mueller A, Berglund RK, Ayyathurai R, Soloway C, Soloway MS, Abouassaly R, Klein EA, Jones SJ, Zappavigna C, Goldenberg L, Scardino PT, Eastham JA, Guillonneau B.University of Chicago, Chicago, Illinois, USA.
PURPOSE: For select men with low risk prostate cancer active surveillance is more often being considered a management strategy. In a multicenter retrospective study we evaluated the actuarial rates and predictors of remaining on active surveillance, the incidence of cancer progression and the pathological findings of delayed radical prostatectomy. MATERIALS AND METHODS: A cohort of 262 men from 4 institutions met the inclusion criteria of age 75 years or younger, prostate specific antigen 10 ng/ml or less, clinical stage T1-T2a, biopsy Gleason sum 6 or less, 3 or less positive cores at diagnostic biopsy, repeat biopsy before active surveillance and no treatment for 6 months following the repeat biopsy. Active surveillance started on the date of the second biopsy. Actuarial rates of remaining on active surveillance were calculated and univariate Cox regression was used to assess predictors of discontinuing active surveillance.
RESULTS: With a median followup of 29 months 43 patients ultimately received active treatment. The 2 and 5-year probabilities of remaining on active surveillance were 91% and 75%, respectively. Patients with cancer on the second biopsy (HR 2.23, 95% CI 1.23-4.06, p = 0.007) and a higher number of cancerous cores from the 2 biopsies combined (p = 0.002) were more likely to undergo treatment. Age, prostate specific antigen, clinical stage, prostate volume and number of total biopsy cores sampled were not predictive of outcome. Skeletal metastases developed in 1 patient 38 months after starting active surveillance. Of the 43 patients undergoing delayed treatment 41 (95%) are without disease progression at a median of 23 months following treatment.
CONCLUSIONS: With a median followup of 29 months active surveillance for select patients appears to be safe and associated with a low risk of systemic progression. Cancer at restaging biopsy and a higher total number of cancerous cores are associated with a lower likelihood of remaining on active surveillance. A restaging biopsy should be strongly considered to finalize eligibility for active surveillance.
http://www.ncbi.nlm.nih.gov/pubmed/15839912
BJU Int. 2005 May;95(7):956-60.
Early outcomes of active surveillance for localized prostate cancer.
Hardie C, Parker C, Norman A, Eeles R, Horwich A, Huddart R, Dearnaley D.
Academic Unit of Radiotherapy & Oncology, The Royal Marsden NHS Trust and Institute of Cancer Research, Sutton, Surrey, UK.
OBJECTIVE: To describe the preliminary clinical outcomes of active surveillance (AS), a new strategy aiming to individualize the management of early prostate cancer by selecting only those men with significant cancers for curative therapy, and illustrate the contrast with a policy of watchful waiting (WW). PATIENTS AND METHODS: Eighty men with early prostate cancer began AS at the authors’ institution between 1993 and 2002. Eligibility included histologically confirmed prostatic adenocarcinoma, fitness for radical treatment, clinical stage T1/T2, N0/X, M0/X, a prostate specific antigen (PSA) level of < or = 20 ng/mL, and a Gleason score of < or = 7. PSA was measured and a digital rectal examination conducted at 3-6 month intervals. The decision between continued monitoring or radical treatment was informed by the rate of rise of PSA, and was made according to the judgement of each patient and clinician. During the same period, 32 men with localized prostate cancer (any T stage, N0/X, M0/X, any PSA, Gleason score < or = 7) were managed by WW; hormonal treatment was indicated for symptomatic prostate cancer progression. The PSA doubling time (DT) was calculated using linear regression of ln(PSA) against time, using all pretreatment PSA values. RESULTS: At a median follow-up of 42 months, 64 (80%) of the 80 patients on AS remained under observation, 11 (14%) received radical treatment and five (6%) died from other causes. No patient developed evidence of metastatic disease, none started palliative hormone therapy, and there were no deaths from prostate cancer. Of the 11 patients who received radical treatment all remained biochemically controlled with no clinical evidence of recurrent disease. The median PSA DT while on AS was 12 years. Twenty (62%) of the 32 patients on WW remained on observation, eight (25%) received palliative hormonal therapy and four (12%) died, including one from prostate cancer. CONCLUSIONS: AS is feasible in selected men with early prostate cancer. The natural history of this disease often appears extremely indolent, and most men on AS will avoid radical treatment. There is a marked contrast between AS (with radical treatment for biochemical progression) and WW (with palliative treatment for symptomatic progression). Ongoing studies are seeking to optimize the AS protocol, and to compare the long-term outcomes with those of immediate radical treatment.
http://www3.interscience.wiley.com/cgi-bin/fulltext/119142464/HTMLSTART
Role of repeated biopsy of the prostate in predicting disease progression in patients with prostate cancer on active surveillance
Mohammed Al Otaibi, MD 1, Philip Ross, MD 1, Nader Fahmy, MD 1, Suganthiny Jeyaganth, MsC 1, Helen Trottier, PhD 2, Kanishka Sircar, MD 3, Louis R. Bégin, MD 3, Luis Souhami, MD 4, Wassim Kassouf, MD 1, Armen Aprikian, MD 1, Simon Tanguay, MD 1 *
The prevalence of prostate cancer in men aged >50 years has been estimated to be as high as 40%
A large proportion of these cancers are potentially insignificant and if left untreated may not necessarily impact an individual patient’s survival or quality of life
Many patients with potentially insignificant tumors are interested in the concept of active surveillance with delayed intervention. Although attractive, this approach is only feasible if we are able to clearly identify patients when their disease is changing. The challenge remains to accurately identify those men with an aggressive, localized prostate cancer, which has the potential to impact survival if left untreated, while sparing or delaying treatment to avoid the morbidity of a treatment that may not change the natural history of the disease.
patients on AS must accept frequent and regular evaluations of the status of their cancer for as long as they remain potential candidates for definitive therapy. Of the various parameters monitored in these men, pathologic findings on prostate biopsy remain the most objective measures of the evolution of their cancer.
Diagnostic PSA values, including free and total levels, were examined by several investigators including ourselves and were not found to be helpful in the identification of men who require therapy.[16-23] Conversely, PSADT has been shown to be a predictor of disease progression. Choo et al.[18] suggested that the definition of disease progression for men on AS include a PSADT of <2 years on the basis of at least 3 separate PSA measurements during a minimum of 6 months. However, in their series using these criteria, 6 of 9 men who underwent RP had extraprostatic disease, suggesting that this PSADT threshold may be too short to effectively identify patients at risk of disease progression. In our cohort, only 5 patients had a PSADT of <2 years and 3 of these patients demonstrated pathologic disease progression. The results of the current study demonstrated that a PSADT of <67 months was associated with an increased risk of pathologic disease progression. Patel et al.[24] did not find a correlation between PSADT and disease progression in their series.
Pathologic disease progression was most often defined by an increase in tumor volume, whereas only 5 patients (15%) were considered to have disease progression as a result of Gleason pattern upgrading to 4. Pathologic findings of any cores involved with >20% of cancer at the time of diagnosis or 2 cores positive for cancer at the time of diagnosis were associated with an increased risk of disease progression. The results of the current study demonstrated that the absence of cancer on repeated core needle biopsy early after initial diagnosis identified those patients who were less likely to develop disease progression. Patel et al.[24] and Carter et al.[25] reported a similar association between the results of first repeated biopsy and the risk of disease progression.
Therefore, we strongly recommend considering treatment in men on AS who demonstrate cancer on repeat biopsy. When pathologic disease progression was observed on follow-up rebiopsy
http://www.ncbi.nlm.nih.gov/pubmed/16713065
Eur Urol. 2006 Sep;50(3):475-82. Epub 2006 May 3.
Management and survival of screen-detected prostate cancer patients who might have been suitable for active surveillance. Roemeling S, Roobol MJ, Postma R, Gosselaar C, van der Kwast TH, Bangma CH, Schröder FH.Department of Urology, Erasmus MC, University Medical Center, Rotterdam, The Netherlands.
OBJECTIVE: Screening practices for prostate cancer have resulted in an increasing incidence of prostate cancers. Our knowledge about which prostate cancers are life threatening and which are not is limited. Thus, for ethical, medical, and economic reasons we need to define which patients can be managed by active surveillance. METHODS: From 1993 through 1999, men from the Rotterdam section of the European Randomized study of Screening for Prostate Cancer (ERSPC) were screened by two strict protocols, which were based on prostate-specific antigen (PSA), digital rectal examination, and transrectal ultrasound. For this study, men with criteria that reflect current active surveillance studies were selected: those with a biopsy Gleason score < or =3+3 in two or fewer cores, with a PSA density <0.2 and a maximum PSA-level of 15 ng/ml. Clinical stage had to be T1C or T2. RESULTS: Of the 1,014 prostate cancers detected in the prevalence screen, 293 men (28.9%) met the criteria for active surveillance. Their mean age was 65.7 and the mean PSA level was 4.8 ng/ml. Radical prostatectomy was elected by 136 men (46.4%), radiotherapy by 91 (31.1%), and watchful waiting by 64 (21.8%). The mean follow-up was 80.8 months. The eight-year prostate cancer-specific survival was 99.2%; the overall survival was 85.4%. Nineteen men who chose watchful waiting changed to definitive treatment during follow-up. CONCLUSION: Only three men died of prostate cancer, none of whom were on watchful waiting. Our observations provide preliminary validation of the arbitrary selection criteria for active surveillance.
http://www.ncbi.nlm.nih.gov/pubmed/18387385
Urology. 2008 Apr;71(4):573-7. Links
Staging saturation biopsy in patients with prostate cancer on active surveillance protocol.
Abouassaly R, Lane BR, Jones JS.
Glickman Urological Institute, Cleveland Clinic, Cleveland, Ohio 44195, USA.
OBJECTIVES: One option for the management of low-grade, low-stage prostate cancer is to delay or forego treatment unless evidence of an increased risk of disease progression exists. Accurate assessment of the disease extent and aggressiveness is necessary to determine the candidates for active surveillance (AS). Office-based saturation prostate biopsy (S provides more accurate staging than traditional biopsy; therefore, we studied its role in patients on an AS protocol. METHODS: Our database identified 52 men with prostate cancer treated with AS from July 2000 to May 2007. The records were reviewed to determine the role of SB in determining the need for definitive therapy. RESULTS: The patients had a median age of 69 years (range 51 to 83) and median prostate-specific antigen (PSA) level of 5.1 ng/mL (range 0.5 to 47). Patients underwent subsequent staging 20-core SB a median of 9 months (range 1 to 20 months) after diagnosis. The disease of 20 patients (38%) was upstaged as defined by an increase in Gleason score or increased disease volume, leading to a recommendation for active treatment. Patients with disease upstaging had had significantly fewer cores taken at the initial diagnostic biopsy (11% with 20 cores or more compared with 55% with fewer than 20 cores, P = 0.002). CONCLUSIONS: SB might lead to a more accurate assessment of the extent and grade of disease in men with prostate cancer on an AS protocol than traditional biopsy. In our series, more than one half of patients who pursue an AS protocol delayed or avoided local therapy. No patient developed clinical metastasis, but long-term surveillance is required.
http://www3.interscience.wiley.com/cgi-bin/fulltext/114132008/HTMLSTART
Prostate-specific antigen velocity and prostate cancer gleason grade and stage
Paul F. Pinsky, PhD 1 *, Gerald Andriole, MD 2, E. David Crawford, MD 3, David Chia, MD 4, Barnett S. Kramer, MD 5, Robert Grubb, MD 2, Robert Greenlee, PhD 6, John K. Gohagan, PhD 1 1Division of Cancer Prevention, National Cancer Institute, Bethesda, Maryland
Prostate cancer staging
http://en.wikipedia.org/wiki/Prostate_cancer_staging
From the AJCC 6th edition (2002) and UICC 6th edition.
NUTRITIONAL APPROACH
http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pubmed&pubmedid=18044088
Clin Interv Aging. 2007 March; 2(1): 153–161.
Published online 2007 March. PMCID: PMC2684075
Is it necessary to cure prostate cancer when it is possible?
(Understanding the role of prostate inflammation resolution to prostate cancer evolution)
Ronald E Wheeler Prostatitis & Prostate Cancer Center, Sarasota, Fl, USA Ronald E Wheeler, The Prostate Cancer Center, 1250 South Tamiami Trail, Suite One North, Sarasota, Florida 34239, USA, Tel +1 941 957 0007,
In 2005, the incidence of prostate cancer was noted to be in excess of 232 000 new cases
with approximately 32 000 men dying from the disease (ACS 2004). According to the SEER (Surveillance, Epidemiology & End Result) data and the age specific population projections in association with the United States Census Bureau, it is estimated that 99 000 men will die from prostate cancer in the year 2045 (Chan et al 2004). Besides the health risk, there is also concern about the best way to pay for expensive prostate cancer treatment in the future where an aging population is expected to exhibit high rates of prostate cancer detection (Fowler et al 2000). Despite our best efforts to cure, failure rates for prostate cancer may be as high as 40%–60% in high-risk cases (Tefilli et al 1999).
Description of the patented prostatitis formula
Peenuts® is a standardized formula for prostate health readily available around the world. The formula is a proprietary blend of vitamins, minerals, amino acids, and beta sitosterols. The following ingredients make up this formula:
•Vitamins–C, B6, E
•Minerals–zinc, selenium,
•Herbs–Saw palmetto, Pygeum africanum, stinging nettle, pumpkin seed, Echinacea purpurea, garlic, ginkgo biloba
•Amino acids–L-glycine, L-alanine, L-glutamic acid.
Modified Mediterranean Diet
The Modified Mediterranean Diet encompasses all of the traditional components of a standard Mediterranean Diet including fresh fruits and vegetables, olive oil, Omega 3 fatty acids, fish, tomato and tomato-related products, and red wine. The modification to this diet comes with a limitation of pasta as well as an avoidance of red meat and dairy fat associated with a fatty acid called Arachidonic acid found in the saturated fats of these food items. Based on references sited in the bibliography, Arachidonic acid has been shown to cause prostate cancer to grow aggressively in vitro.
DON’T BIOPSY UNLESS PSA VELOCITY above 1.25 ng/ml per year
Using PSA velocity of 1.25 ng/ml per year to recommend biopsy.
http://www3.interscience.wiley.com/cgi-bin/fulltext/116321833/HTMLSTART
Prostate-specific antigen velocity and the detection of gleason score 7 to 10 prostate cancer
Rinaa S. Punglia, MD, MPH 1 *, Jennifer Cullen, PhD, MPH 2, David G. McLeod, MD 3, Yongmei Chen, MD, MPH 2, Anthony V. D’Amico, MD, PhD 1
Volume 110, Issue 9, Pages 1973-1978. 20 Sep 2007 American Cancer Society
Current standards of practice advocate recommending prostate biopsy when PSA velocity
exceeds 0.75 ng/mL per year.[8]
However, we have demonstrated that using a threshold of 1.0 ng/mL per year or 1.25 ng/mL per year
sacrifices little sensitivity in terms of detection of high-grade disease and reduces the number of biopsies in which no cancer or low-grade disease is identified.
we limited our sample to men who had PSA levels >4 ng/mL
INCREASED SUICIDE IN MEN DX W/ PROSTATE CANCER 4X
Llorente MD, Burke M, Gregory GR, et al. Prostate cancer: a significant risk factor for late-life suicide. Am J Geriatr Psychiatry. 2005; 13: 195-201. Links
Ki-67
http://www.ncbi.nlm.nih.gov/pubmed/18762814
Prostate Cancer Prostatic Dis. 2009;12(2):143-7. Epub 2008 Sep 2. Links
Biopsy tissue microarray study of Ki-67 expression in untreated, localized prostate cancer managed by active surveillance. Jhavar S, et al
Gleason Score Upshifting
http://jnci.oxfordjournals.org/cgi/content/abstract/97/17/1248
JNCI Journal of the National Cancer Institute 2005 97(17):1248-1253; Prostate Cancer and the Will Rogers Phenomenon Peter C. Albertsen, James A. Hanley, George H. Barrows, David F. apparent improvement in mortality held for all Gleason score categories. Conclusions: In this population, a decline in the reported incidence of low-grade prostate cancers appears to be the result of Gleason score reclassification over the past decade. This reclassification resulted in apparent improvement in clinical outcomes. This finding reflects a statistical artifact known as the Will Rogers phenomenon
http://www.forbes.com/2009/08/31/
prostate-cancer-screening-business-healthcare-prostate.html
Medical Tests – The Dark Side Of Prostate Cancer Screening
Robert Langreth, 08.31.09, 04:00 PM EDT PSA tests may lead men into unnecessary treatment, a new study finds.
http://www.cancer.gov/ncicancerbulletin/090809/page2
Study Questions Value of Prostate Cancer Screening
Among the estimated 1.3 million excess prostate cancer diagnoses, slightly more than 1 million men received definitive treatment, such as surgery, hormone therapy, or radiation therapy. “But even using the most optimistic assumption about benefit, the vast majority of these additional 1 million men did not benefit from early detection,” the authors wrote.
A study released online August 31 in the Journal of Clinical Oncology confirms results from earlier studies showing that deferring treatment after prostate cancer diagnosis does not increase the risk of dying from prostate cancer. The study looked at more than 3,000 men diagnosed with prostate cancer between 1986 and 2007. Although only 10 percent of men chose to defer treatment after their initial diagnosis, approximately half still had no definitive treatment after 7 years of follow up. And the death rate from prostate cancer was nearly identical in men who deferred treatment compared with those who chose immediate treatment.
http://www.ncbi.nlm.nih.gov/pubmed/19720918
J Clin Oncol. 2009 Aug 31. [Epub ahead of print] LinksProspective Study of Determinants and Outcomes of Deferred Treatment or Watchful Waiting Among Men With Prostate Cancer in a Nationwide Cohort.Shappley WV 3rd, Kenfield SA, Kasperzyk JL, Qiu W, Stampfer MJ, Sanda MG, Chan JM.Division of Urology, Beth Israel Deaconess Medical Center, and Harvard Medical School; Channing Laboratory, Department of Medicine, Brigham and Women’s Hospital, and Harvard School of Public Health, Boston, MA; and Departments of Epidemiology & Biostatistics and Urology, University of California, San Francisco, San Francisco, CA.
CONCLUSION: In this nationwide cohort, more than half the men who opted for DT remained without treatment for 7.7 years after diagnosis. Older men and men with lesser cancer severity at diagnosis were more likely to remain untreated. PCa mortality did not differ between DT and active treatment patients.
The latest American Cancer Society estimates for prostate cancer in the United States are for 2009: about 192, 280 new cases of prostate cancer will be diagnosed
27,360 men will die of prostate cancer According to the most recent data, for all men with prostate cancer, the relative 5-year survival rate is nearly100% and the relative 10-year survival rate is 91%.
http://www.hemonctoday.com/article.aspx?rid=43778
Researchers reviewed the cases of 14,516 men aged older than 65 who were diagnosed with stage T1 or T2 disease. Data were collected from the SEER database. Three-quarters of the men had Gleason scores between 5 and 7.
The researchers found 10-year disease-specific mortality was 6% (95% CI, 4%-8%) for men in the contemporary PSA era compared with 15% to 23% for men aged 65 to 74 diagnosed with moderately differentiated disease from 1942-1992. The researchers added that survival also improved among older patients and those with poorly differentiated tumors in the contemporary era.
The results also showed that 10-year prostate cancer–specific survival with conservative management has increased from 83% to 87% in the pre-PSA or early PSA era to roughly 94% now, according to the researchers. They also noted that 94% is better than the 90% rate for men treated with prostatectomy during the pre-PSA or early PSA era.
“In summary, our findings suggest that outcomes following conservative management of contemporary PSA- era patients with localized prostate cancer are substantially more favorable than studies from earlier eras,” the researchers wrote. “Patients with well- or moderately differentiated disease managed conservatively are generally even more likely to die of causes other than prostate cancer.” – by Jason Harris
Lu-Yao GL. JAMA. 2009;302:1202-1209.
Like all nonrandomized, retrospective analyses, there is much more we could wish for with these results, but this analysis does provide strong evidence that since the ‘PSA era’ began, the risk of prostate cancer death at 10 years in men with localized disease has improved more than 50% in men with tumors less than Gleason grade 8. These data also emphasize the substantial difference between ‘low-grade’ Gleason tumors, less than 8, and Gleason 8, 9, 10 disease. There are many potential explanations for the improvement in prognosis for men with localized, Gleason less than 8 tumors over time, such as lead-time bias, over-diagnosis and grade migration.
Regardless, this study emphasizes the need to develop indicators of dangerous disease that complement our limited markers and should remind physicians and patients that in patients with an expected life expectancy greater than 10 years and a localized prostate cancer with a Gleason score less than 8, active surveillance/expectant management is a very viable option.
http://jama.ama-assn.org/cgi/content/short/302/11/1202?home
CLINICIAN’S CORNER
Outcomes of Localized Prostate Cancer Following Conservative Management
Grace L. Lu-Yao, MPH, PhD; Peter C. Albertsen, MD; Dirk F. Moore, PhD; Weichung Shih, PhD; Yong Lin, PhD; Robert S. DiPaola, MD; Michael J. Barry, MD; Anthony Zietman, MD; Michael O’Leary, MD, MPH; Elizabeth Walker-Corkery, MPH; Siu-Long Yao, MD
JAMA. 2009;302(11):1202-1209.
Context Most newly diagnosed prostate cancers are clinically localized, and major treatment options include surgery, radiation, or conservative management. Although conservative management can be a reasonable choice, there is little contemporary prostate-specific antigen (PSA)–era data on outcomes with this approach.
Objective To evaluate the outcomes of clinically localized prostate cancer managed without initial attempted curative therapy in the PSA era.
Design, Setting, and Participants A population-based cohort study of men aged 65 years or older when they were diagnosed (1992-2002) with stage T1 or T2 prostate cancer and whose cases were managed without surgery or radiation for 6 months after diagnosis. Living in areas covered by the Surveillance, Epidemiology, and End Results (SEER) program, the men were followed up for a median of 8.3 years (through December 31, 2007). Competing risk analyses were performed to assess outcomes.
Main Outcome Measures Ten-year overall survival, cancer-specific survival, and major cancer related interventions.
Results Among men who were a median age of 78 years at cancer diagnosis, 10-year prostate cancer-specific mortality was 8.3% (95% confidence interval [CI], 4.2%-12.8%) for men with well-differentiated tumors; 9.1% (95% CI, 8.3%-10.1%) for those with moderately differentiated tumors, and 25.6% (95% CI, 23.7%-28.3%) for those with poorly differentiated tumors. The corresponding 10-year risks of dying of competing causes were 59.8% (95% CI, 53.2%-67.8%), 57.2% (95% CI, 52.6%-63.9%), and 56.5% (95% CI, 53.6%-58.8%), respectively. Ten-year disease-specific mortality for men aged 66 to 74 years diagnosed with moderately differentiated disease was 60% to 74% lower than earlier studies: 6% (95% CI, 4%-8%) in the contemporary PSA era (1992-2002) compared with results of previous studies (15%-23%) in earlier eras (1949-1992). Improved survival was also observed in poorly differentiated disease. The use of chemotherapy (1.6%) or major interventions for spinal cord compression (0.9%) was uncommon.
Conclusions Results following conservative management of clinically localized prostate cancer diagnosed from 1992 through 2002 are better than outcomes among patients diagnosed in the 1970s and 1980s. This may be due, in part, to additional lead time, overdiagnosis related to PSA testing, grade migration, or advances in medical care.
http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pubmed&pubmedid=17077805
Br J Cancer. 2006 November 6; 95(9): 1186–1194.
Long-term outcome among men with conservatively treated localised prostate cancer
J Cuzick,1,9* G Fisher,1 M W Kattan,2 D Berney,3 T Oliver,4 C S Foster,5 H Møller,6 V Reuter,7 P Fearn,8 J Eastham,8 and P Scardino8,9 Received May 15, 2006; Revised August 10, 2006; Accepted August 10, 2006.
The first randomised trial of primary treatment with curative intent for men with localised prostate cancer was reported by Holmberg et al (2002) and later by Bill-Axelson et al (2005). This trial included 695 men, with clinically localised prostate cancer, randomised to either radical prostatectomy or no initial treatment with systemic treatment deferred until the development of symptomatic progression. The authors found a reduced risk of progression and death from prostate cancer in the radically treated men, but concluded that the disease-specific benefits of radical prostatectomy must be weighed carefully against the potential impact that surgery can have on quality of life. Other studies (Chodak et al, 1994; Albertsen et al, 1995, 1998, 2005a; Adolfsson et al, 1997; Holmberg et al, 2002) have concluded that watchful waiting or no initial treatment with treatment delayed until the development of symptomatic metastatic disease remains a viable treatment option. A basic tenet of an effective screening programme is that the natural history of the disease should be understood well and that early detection can have an important impact on outcome. Neither of these requirements has been satisfied for prostate screening.
Jeffrey Dach MD
7450 Griffin Road
Suite 190
Davie, Florida 33314
954-792-4663
http://www.jeffreydach.com/
http://www.drdach.com/
http://www.naturalmedicine101.com/
http://www.truemedmd.com/
Disclaimer click here: http://www.drdach.com/wst_page20.html
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this article:http://wp.me/P3gFbV-8f
http://jeffreydach.com/2009/10/01/psa-testing-the-failed-medical-experiment-by-jeffrey-dach-md.aspx
Copyright (c) 2009 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.








{kind=link}
{kind=link}
PSA Screening for Prostate Cancer the Failed Experiment - Jeffrey Dach MD August 18, 2013 at 11:57 AM
[…] PSA Screening for Prostate Cancer, the Failed Medical Experiment by Jeffrey Dach MD A Case of an Elevated PSA Jim, a 55 year old athlete and outdoors man, who runs marathons and camps out, was not at all worried about prostate cancer until he saw the Larry King Live Show endorsing PSA screening for prostate cancer. Jim into a local Miami hospital offering free screening for prostate cancer….To Read More Click Here […]
The Failed Medical Experiment: PSA Screening for Prostate Cancer August 21, 2013 at 2:22 PM
[…] References for this article can be found at the original source. […]
El experimento médico fallido: la prueba PSA de detección del cáncer de próstata. | Disiciencia August 27, 2013 at 2:26 PM
[…] Para consultar los Links y Referencias ir al artículo original. […]