954-792-4663
 Heartburn, GE Reflux (GERD), and Acid Blocker Drugs
Heartburn, GE Reflux (GERD), and Acid Blocker Drugs
by Jeffrey Dach MD
This article is part one of a series, for part two, click here.
A July 2009 study of Acid Blocker Drugs shocked the medical community, reporting the drugs actually caused the symptoms they are supposed to treat. The study recruited asymptomatic healthy volunteers who took Acid Blocker drugs for a few weeks, and then stopped. Upon stopping the Acid Blocker drug, more than 40% of the volunteers reported heartburn and acid regurgitation, symptoms they never had until after they stopped the Acid Blocker drug.
(These drugs are Prolisec, Nexium Aciphex, Protonix, and are also called PPI’s for Proton Pump Inhibitors).
Dr Christine Reimer the author, said her study revealed “unrecognized aspects of Acid Blocker -PPI drug withdrawal with acid rebound”.
Left Image: Heartburn, Fire Breathing Man courtesy of Wikimedia commons.
The Acid Blocker Drug Merry-Go-Round
For the typical heartburn relieved with acid blocker drugs, symptoms return with a vengeance when the drug is stopped. This withdrawal effect is the hallmark of an addictive drug, in this case caused by “rebound acid hypersecretion” with increased gastric acid production. The worsening heartburn pain forces the victim to immediately go back on the PPI acid blocker drug, and continue indefinitely into the future.

Left Image: Merry go round courtesy of wikimedia commons.
Windfall Profits from An Addictive Drug
With 5% of the population taking acid blocker PPI drugs, this represents a blockbuster profit for the drug companies. Ask any street corner drug dealer, and they will tell you the best business is the addictive drug business, the clients always return for more.
PPI’s Are As Safe As Placebo
Your doctor probably tells you acid blocker drugs are safe, with no adverse effects. An article in a mainstream medical journal (AAFP) says,” The frequency of adverse effects associated with PPIs is similar to that of placebo”. This is not exactly true as you will see below.

Left Image: Nexium (Purple Pill) courtesy of wikimedia commons.
Adverse Effects of PPI Acid Blocker Usage
The adverse effects of Acid Blocker Drugs are related to the profound reduction in gastric acid. They really do their job well, reducing stomach acid to virtually nothing.
Most of the adverse effects of PPI’s are related to the fact that stomach acid is needed for digestion and absorption of food, in particular key nutrients like B12, calcium, Iron and Protein. The 5% of our population on PPI drugs are at risk for hip fracture, B12 deficiency, amino acid deficiency, and iron deficiency anemia. One study showed reduced cognition from PPI’s.
Secondly, Gastric Acid serves as a defensive barrier to invading bacterial organisms and kills any ingested bacteria, before it can overwhelm the body’s defenses. With stomach acid turned off by the PPI drug, these bacteria are free to invade. This results in increased incidence of pneumonia, as well as Clostridia Difficile Entero-Colitis in patients on PPI’s.
PPI Drugs Cause Gastric Polyps, Paralysis of the Stomach and Gut Dysmotility
Dr A Breck McKay, in a letter to the British Medical Journal, said ” long term use of
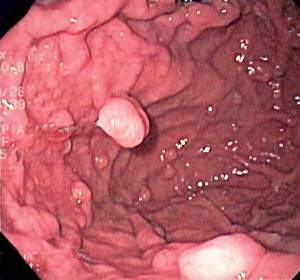
PPIs cause gastroparesis, delayed total gut dysmotility and bloating” Patients suffer acute, explosive, exacerbation of their gastritis and reflux, on attempted cessation of the PPIs. While the PPI drugs block acid production, these drugs actually stimulate hormones like gastrin, cholecystokinin, and glucagon which in turn stimulate growth of acid producing cells to massively increase and thus, are able to produce large quantities of acid, suddenly, when inhibition from the acid blocker PPI drug stops.
Left Image: Endoscopic view of stomach showing Gastric polyps and hyperplastic folds due to PPI drugs. Courtesy wikimedia commons.
Handed Out Like Candy
Nonetheless, PPI drugs are handed out freely, like candy. Dr. Yeomans advised physicians not to “over-react” to concerns about the biological effects of inhibiting acid secretion with proton pump inhibitors.
What Causes GE Reflux and Acid Heartburn?
The cause of reflux is well known. Firstly, there is a mechanical problem with the lower esophageal sphincter (valve) which allows gastric contents to go back up into the lower esophagus. See Image at left of Barium Xray. The white barium has refluxed back up into the esophagus (red arrow). The acidic  gastric contents causes irritation, damage and heartburn pain. Turning off gastric acid with a blocker drug will relieve the symptoms, but does not address the underlying mechanical problems.
gastric contents causes irritation, damage and heartburn pain. Turning off gastric acid with a blocker drug will relieve the symptoms, but does not address the underlying mechanical problems.
Left Image: Xray showing reflux of barium contrast into esophagus (red arrows) courtesy of wikimedia commons.
As a radiologist for 30 years, a large part of my job was taking pictures of GE reflux with barium X-rays. I never saw reflux when the patient was standing up. We were able to induce GE reflux before our eyes merely by placing the patient down in the supine position with the motorized table controls. Now, with the patient in the supine position (lying down) turned back and forth on the table, we then see the reflux on the xray flouriscopic screen, with the barium contrast spilling up from the stomach into the eophagus.
Stay Standing Up or Sitting Up For Three Hours After a Meal.
Whenever I saw the GE reflux, I would then inform the patient they have reflux, and that it is important to stay standing up or sitting up for three hours after they eat a meal. GE reflux cannot occurr in the standing or sitting position. After three hours, the stomach should be empty, so it should be safe sleep for the night.
Eradicate the Helicobacter Pylori
Secondly, there may be a co-existing bacterial infection in the stomach called H. Pylori detected with a simple blood test. Eradiction of the the H Pylori infection with antibiotics is an important step to ending the heartburn/reflux and getting off the PPI Merry Go Round. Thirdly, lifestyle and dietary modifications described below by Dr Hyman are essential to ending the heartburn. Avoid spicy foods, eat smaller meals, do not lie down after meals, stay  standing or sitting up for three hours after a meal.
standing or sitting up for three hours after a meal.
Left Image: H. Pylori bacteria (red arrow) imbedded in stomach lining. Courtesy of wikimedia commons.
Mastic Gum – an Ancient Remedy – Kills H. Pylori
Mastic Gum is an old remedy used for centuries as a chewable gum effective against H Pylori. This is readily available at the health food store. An excellent article on Gum Mastic by Karina L. Gordin appears in the October issue of the Townsend Letter. She interviewed Dr Leo Galland who recommended Mastic Gum in capsule form (1000 mg twice a day) to a patient with gastritis. Not only did the gastritis clear up, underlying ulcerative colitis also went into full remission. A 1998 landmark article in the New England Journal of Medicine on Mastic Gum, showing activity against H Pylori, is largely responsive for renewed interest in this old remedy. See references below for more on Mastic Gum.
Simple Steps to Get Off Your Acid Blocking Drug
This 7 minute video by Mark Hyman MD is an excellent summary:
3 Simple Steps to Eliminate Heartburn and Acid Reflux by Mark Hyman MD
The H. Pylori Story, The Nobel Prize and The Eradication of Gastric Ulcers
The Disappearing Gastric Ulcer
Left image: The Disappearing Ulcer. Barium X-Ray showing typical appearance of benign gastric ulcer (red arrow) with classical radiating folds. Triple therapy has eliminated this. Courtesy of Wikimedia Commons.
 The 2005 Nobel prize was awarded to Barry J. Marshall and J. Robin Warren for the recognition of H. Pylori infection as the causative agent in gastric and duodenal ulcrs. With this great discovery, medical science is now able to cure gastric and duodenal ulcers by eradicating the H Pylori bacterial infection. This is done with “Triple Therapy” consisting of two antibiotics and a PPI acid blocker drug. Once the ulcer is cured, treatment is discontinued.
The 2005 Nobel prize was awarded to Barry J. Marshall and J. Robin Warren for the recognition of H. Pylori infection as the causative agent in gastric and duodenal ulcrs. With this great discovery, medical science is now able to cure gastric and duodenal ulcers by eradicating the H Pylori bacterial infection. This is done with “Triple Therapy” consisting of two antibiotics and a PPI acid blocker drug. Once the ulcer is cured, treatment is discontinued.
Left Image: A Rare Bird, Gone Away. Endoscopic view of benign gastric ulcer crater (center) with typical radiating folds. Courtesy of wikimedia commons.
Changes During My Radiology Career
When I started out as at the beginning of my career as a radiologist in 1976, Gastric and Duodenal ulcers were quite  common, and a large part of my job was using Xray imaging to make the diagnosis. I found many ulcers in my day. Not any more. Triple therapy for H. Pylori has made gastric and duodenal ulcers ancient history, these are now quite rare, an ancient relic of the past, destined for the medical museum. (link)
common, and a large part of my job was using Xray imaging to make the diagnosis. I found many ulcers in my day. Not any more. Triple therapy for H. Pylori has made gastric and duodenal ulcers ancient history, these are now quite rare, an ancient relic of the past, destined for the medical museum. (link)
Left Image: A Photo for the Museum showing a typical Duodenal Ulcer crater (red arrow) on air contrast upper GI X-Ray. Contrast agent is barium and effervescent CO2 crystals. We rarely see these any more. Courtesy Wikimedia Commons.
The Truth About Acid Reflux by Suzy Cohen, RPh Published on  Mar 16, 2013 http://www.DearPharmacist.com You may be taking an acid blocking drug or antacid and not even need it. Watch this video to learn the truth about WHY acid reflux happens. watch video below….
Mar 16, 2013 http://www.DearPharmacist.com You may be taking an acid blocking drug or antacid and not even need it. Watch this video to learn the truth about WHY acid reflux happens. watch video below….
———————————-
Buy Digestive Enzymes Ultra with Betaine HCL from Purecaps
Buy Betaine HCL with Pepsinon Amazon
Articles With related Interest:
This article is part one of a series, for Part Two CLick Here.
Hair Loss From Low Stomach Acid, the Lady in Grey
Jeffrey Dach MD
7450 Griffin Road Suite 190
Davie, Florida 33314
954-792-4663
http://www.jeffreydach.com/
http://www.drdach.com/
http://www.naturalmedicine101.com/
http://www.truemedmd.com/
http://www.bioidenticalhormones101.com/
Links and References:
PPI’s Promote Dependency and Addiction
http://www.gastrojournal.org/article/S0016-5085(09)00522-8/fulltext
Gasteroenterology – Volume 137, Issue 1, Pages 80-87.e1 (July 2009) Proton-Pump Inhibitor Therapy Induces Acid-Related Symptoms in Healthy Volunteers After Withdrawal of Therapy Christina Reimer, Bo Søndergaard, Linda Hilsted‡, Peter Bytzer
http://www.gastrojournal.org/article/S0016-5085(09)00780-X/fulltext
Evidence That Proton-Pump Inhibitor Therapy Induces the Symptoms it Is Used to Treat , 01 June 2009 Kenneth E.L. McColl, Derek Gillen Gastroenterology July 2009 (Vol. 137, Issue 1, Pages 20-22)
http://www.ncbi.nlm.nih.gov/pubmed/10848649
Aliment Pharmacol Ther. 2000 Jun;14(6):651-68.
Review article: potential gastrointestinal effects of long-term acid suppression with proton pump inhibitors. Laine L, Ahnen D, McClain C, Solcia E, Walsh JH.
http://www.gastro.org/wmspage.cfm?parm1=7371
Science News- Acid-Reducing Medicines May Lead to Dependency
Data suggests proton pump inhibitors can induce acid-related symptoms in healthy adults
Bethesda, MD (July 1, 2009) – Treatment with proton pump inhibitors (PPIs) for eight weeks induces acid-related symptoms like heartburn, acid regurgitation and dyspepsia once treatment is withdrawn in healthy individuals, according to a new study in Gastroenterology, the official journal of the American Gastroenterological Association (AGA) Institute.
“The observation that more than 40 percent of healthy volunteers, who have never been bothered by heartburn, acid regurgitation or dyspepsia, develop such symptoms in the weeks after cessation of PPIs is remarkable and has potentially important clinical and economic implications,” said Christina Reimer, MD, of Copenhagen University and lead author of the study. “This study indicates unrecognized aspects of PPI withdrawal and is a very strong indication of a clinically significant acid rebound phenomenon that needs to be investigated in proper patient populations.”
http://heartburn.about.com/b/2009/07/01/256382.htm
PPIs May Induce Reflux Symptoms & Become Addictive -Wednesday July 1, 2009
According to a new study, published in the Journal of Gastroenterology, proton pump inhibitors (PPIs) can become addictive, and may even induce the symptoms that they were designed to treat. Christina Reimer, MD of Copenhagen University and lead author of the study, stated, “The observation that more than 40 percent of healthy volunteers, who have never been bothered by heartburn, acid regurgitation or dyspepsia, develop such symptoms in the weeks after cessation of PPIs is remarkable and has potentially important clinical and economic implications. This study indicates unrecognized aspects of PPI withdrawal and is a very strong indication of a clinically significant acid rebound phenomenon that needs to be investigated in proper patient populations.”
http://www.medicinenet.com/script/main/art.asp?articlekey=101718
Study: Acid Reflux Drugs Cause Rebound Symptoms
PPI’s and HIP Fracture
http://jama.ama-assn.org/cgi/content/abstract/296/24/2947
Vol. 296 No. 24, December 27, 2006 JAMA
Long-term Proton Pump Inhibitor Therapy and Risk of Hip Fracture
Yu-Xiao Yang, MD, MSCE; James D. Lewis, MD, MSCE; Solomon Epstein, MD; David C. Metz, MD
JAMA. 2006;296:2947-2953.
Context Proton pump inhibitors (PPIs) may interfere with calcium absorption through induction of hypochlorhydria but they also may reduce bone resorption through inhibition of osteoclastic vacuolar proton pumps. Long-term PPI therapy, particularly at high doses, is associated with an increased risk of hip fracture.
PPI’s and B12 Malabsorption
http://www.annals.org/cgi/content/abstract/120/3/211
Omeprazole Therapy Causes Malabsorption of Cyanocobalamin (Vitamin B12)
Stefan P. Marcuard; Lisa Albernaz; and Prabhaker G. Khazanie – Annals of Internal Med February 1994, Volume 120. Issue 3, Pages 211-215 Results: At the end of the 2-week treatment period, cyanocobalamin absorption decreased from 3.2% to 0.9% (P = 0.031) in participants receiving 20 mg of omeprazole daily. In patients taking 40 mg of omeprazole daily, cyanocobalamin absorption decreased from 3.4% to 0.4% (P < 0.05).
Conclusions: Omeprazole therapy acutely decreased cyanocobalamin absorption in a dose-dependent manner.
PPI’s and Pneumonia
http://archinte.ama-assn.org/cgi/content/abstract/167/9/950
Gulmez SE, Holm A, Frederiksen H, Jensen TG, Pedersen C, Hallas J. Use of proton pump inhibitors and the risk of community-acquired pneumonia: a population-based case-control study. Arch Intern Med 2007;167:950-5.
Use of Proton Pump Inhibitors and the Risk of Community-Acquired Pneumonia
A Population-Based Case-Control Study – Sinem Ezgi Gulmez, MD, PhD; Anette Holm, MD, PhD; Henrik Frederiksen, MD, PhD; Thøger Gorm Jensen, MD, PhD; Court edersen, DMSC; Jesper Hallas, DMSC
Arch Intern Med. 2007;167(9):950-955. Conclusion The use of PPIs, especially when recently begun, is associated with an increased risk of community-acquired pneumonia.
Adverse Side Effects of PPI’s on Wikipedia
Clostridium Difficile Diarrhea
http://en.wikipedia.org/wiki/Omeprazole
Side effects- Some of the most frequent side effects of omeprazole (experienced by over 1% of those taking the drug) are headache, diarrhea, abdominal pain, nausea, dizziness, trouble awakening and sleep deprivation, although in clinical trials the incidence of these effects with omeprazole was mostly comparable to that found with placebo.[2]
Proton pump inhibitors may be associated with a greater risk of hip fractures,[3] and clostridium difficile-associated diarrhea.[4] Patients are frequently administered the drugs in intensive care as a protective measure against ulcers, but this use is also associated with a 30% increase in occurrence of pneumonia.[5] Other side effects may include bone rebuild interference and B12 vitamin reduction.[citation needed]
Proton pump inhibitors and Clostridium difficile. Bandolier. 2003. http://www.medicine.ox.ac.uk/bandolier/booth/Pharmacy/PPIcdiff.html
Shoshana J. Herzig, MD; Michael D. Howell, MD, MPH; Long H. Ngo, PhD; Edward R. Marcantonio, MD, SM (2009). Acid-Suppressive Medication Use and the Risk for Hospital-Acquired Pneumonia . JAMA the Journal of the American Medical Association 301 (20): 2120–2128. doi:10.1001/jama.2009.722. PMID 19470989.
http://jama.ama-assn.org/cgi/content/abstract/301/20/2120
Acid Blockers Cause Reduced Cognition
http://www.ncbi.nlm.nih.gov/pubmed/17661965
Boustani, M. The Association Between Cognition and Histamine-2 Receptor Antagonists in African Americans. Journal of the American Geriatrics Society, August 2007; Vol 55: pp. 1248
CONCLUSION: H2As might be a risk factor for the development of cognitive impairment in African Americans. This finding requires confirmation from future studies.
BMJ Editorial on OverPrescribing PPI’s
http://www.bmj.com/cgi/content/full/336/7634/2
BMJ 2008;336:2-3 (5 January), Overprescribing proton pump inhibitors – Is expensive and not evidence based
Letters to BMJ
http://www.bmj.com/cgi/eletters/336/7634/2#185858
“We have become increasingly concerned about the long term side effects being identified in General Practice/Surgery patients, with the current extensive, long term use of the proton pump inhibitors (PPIs). We now share an increasing number of patients with dependence on the PPIs, who experience acute, severe gastritis and gastro-oesophageal reflux, if they suddenly stop or miss their PPIs and some are now displaying refractory gastroparesis and severely delayed jejuno-ileal and colonic peristalsis on trying to reduce or stop their PPI medication , when the PPI has been in use for extended periods (>3 to 60 months).
Three example patients, all under 46 and very fit, developed reflux and gastritis, and following long term use of PPIs (36-60 months), have all developed refractory-to-cisapride, gastroparesis and delayed total gut dysmotility and bloating, (repeatedly shown by all investigative modalities), and they suffer acute, explosive, exacerbation of their gastritis and reflux, on attempted cessation of the PPIs. All have been offered “corrective surgery” for their conditions, which are now identified as physiologically explainable, side effects of long term PPI use.
Since the PPIs block the normal homeostasis of the gastro-jejuno- ileal-colonic function, (due to their very specific, acid production blocking only, cellular-molecular actions*); this allows the multiple secondary interdependent hormonal levels to increase/decrease out of control and thus the parietal cells massively increase their cell surface membrane folds (x7-14), until they appear fan-like on the gastric surface, and thus increases their ability to produce sudden large quantities of acid, when the PPI stops.
This results in a Zollinger- Ellison like syndrome and the patients restart their PPIs or even increase the dose, compounding the situation!
As medical practitioners we must return to review and apply our basic medical sciences knowledge, to realise the harm that is occurring to our patients from our treatments and we must consider reducing PPI medications by very gradual steps, (as we have to do with the steroids); and question the drive by pharmaceutical companies pursuit of ever better dollar producing drugs, (via funding of research) that do more harm, parallel to their good; to the total human, when such basic homeostatic systems are forgotten or ignored.
* ( The PPIs only block the cellular/molecular acid production and allow secondary build up or excessive reduction of the hormones gastrin, cholecystokinin, secretin, glucagon, motilin, VIP, substance P, somatostatin and other biologically active polypetides, which changes all the homeostasis processes of the whole gastro-intestinal system).
Dr A Breck McKay, Family Physician and Professor Daryl Wall Director of Surgery Princess Alexandra Hospital Ipswich Road BRISBANE Australia.
Images
http://myweb.lsbu.ac.uk/dirt/museum/margaret/722-255-2320420.jpg
http://myweb.lsbu.ac.uk/dirt/museum/728-3212a.html
gastric ulcer
http://www.learningradiology.com/archives06/COW%20184-Gastric%20ulcer-benign/gastriculcercorrect.htm
verview”>http://emedicine.medscape.com/article/36787verview
http://commons.wikimedia.org/wiki/File:Gastric_hyperplastic_polyp_(1)_foveolar_type.jpg
The Vanishing Gastric Ulcer after PPI’s introduced
http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pubmed&pubmedid=19379513
BMC Gastroenterol. 2009; 9: 25. Published 2009 April 20.
Decreasing incidence of peptic ulcer complications after the introduction of the proton pump inhibitors, a study of the Swedish population from 1974–2002. Michael Hermansson,1 Anders Ekedahl,2 Jonas Ranstam,3 and Thomas Zilling. We report a significant decrease in peptic ulcer complications in the Swedish population over the last two decades.
PPI’s also Reduce the Incidence of the NSAID induced Ulcer
http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pubmed&pubmedid=17521422
Arthritis Res Ther. 2007; 9(3): R52. 2007 May 23. Vonkeman et al.;
Proton-pump inhibitors are associated with a reduced risk for bleeding and perforated gastroduodenal ulcers attributable to non-steroidal anti-inflammatory drugs: a nested case-control study. Harald E Vonkeman,1 Robert W Fernandes,2 Job van der Palen,3 Eric N van Roon,4 and Mart AFJ van de Laar1
Long Term Safety of PPI’s
H Pylori eradication eliminated need for long term PPI’s for Ulcers
Long term PPI’s is now used exclusively for GE reflux.
http://www.ncbi.nlm.nih.gov/pubmed/12904157
Expert Opin Drug Saf. 2002 May;1(1):29-38. Long-term safety of proton pump inhibitors: risks of gastric neoplasia and infections.Waldum HL, Brenna E, Sandvik AK.
After Helicobacter pylori eradication was introduced and largely eliminated the need for maintenance therapy for peptic ulcer disease, gastroesophageal reflux disease (GERD) became the main indication for prolonged gastric acid inhibition. The drug effect on GERD depends on the degree of acid inhibition, thus the efficacious proton pump inhibitors are preferred. The proton pump inhibitors have few immediate side effects, the main concern being the profound hypoacidity and hypergastrinaemia they induce. In short-term, hypergastrinaemia causes rebound hyperacidity, possibly worsening GERD and reducing the efficacy of histamine H(2) blockers. In the long-term, hypergastrinaemia causes enterochromaffin-like cell hyperplasia and carcinoids. Since enterochromaffin-like cells may be important in gastric carcinogenesis, iatrogenic hypergastrinaemia may predispose to carcinoma. Gastric hypoacidity also increases gut bacterial infections, and the barrier function of acid against viral and prion infections requires further assessment.
Concern about safety of PPI’s “Over-Reaction”
http://www.ncbi.nlm.nih.gov/pubmed/10735918
Aliment Pharmacol Ther. 2000 Mar;14(3):267-71.
Personal review: alarmism or legitimate concerns about long-term suppression of gastric acid secretion? Yeomans ND, Dent J. Department of Medicine, Western Hospital, Melbourne, Australia.
This article responds to controversial issues about the long-term use of acid suppression raised in a recent article in this journal by Waldum & Brenna. Although rebound acid secretion occurs following proton pump inhibitor therapy, the clinical significance of this is unclear, but the proposal that this is a major driver of acid-related diseases is considered implausible. The polypoid deformity of the gastric corpus that can occur with long-term proton pump inhibitor therapy is not neoplastic, and therefore has no bearing on other issues raised about proton pump inhibitor therapy and gastric malignancy. Current data in humans suggest that the magnitude of serum gastrin elevation from proton pump inhibitor treatment of up to 10 years, and any theoretical risks from this, have been overstated by Waldum & Brenna. Pernicious anaemia is a model of very doubtful validity for the risks of proton pump inhibitor therapy on several grounds. The proposal that diffuse gastric carcinoma arises from acid suppression-induced stimulation of enterochromaffin-like cells is challenged vigorously, because this is based on an implausible and substantially criticized interpretation of histopathology. It is agreed that it is appropriate to be cautious about the safety of long-term acid suppression, because no data are available for lifelong treatment in humans. Such caution should be tempered by a critical assessment of the benefits of this treatment in relation to any possible risks. The substantial data that now exist from long-term treatment of humans with proton pump inhibitors has not thus far revealed any definite risks. The risk of death from anti-reflux surgery, although small, would seem to far exceed any possible risks associated with long-term proton pump inhibitor use. Available data suggest that denial of the benefits of effective acid suppressant therapy to patients with clear-cut troublesome acid related disorders is an overreaction to concerns about the biological effects of inhibiting acid secretion with proton pump inhibitors.
http://www.ncbi.nlm.nih.gov/pubmed/16433886
Basic Clin Pharmacol Toxicol. 2006 Jan;98(1):4-19. Consequences of long-term proton pump blockade: insights from studies of patients with gastrinomas. Jensen RT.
Proton pump inhibitors are being increasingly used and for longer periods of time, especially in patients with gastroesophageal reflux disease.
Potential areas of concern that have been raised in the long-term use of proton pump inhibitors, include: gastric carcinoid formation; rebound acid hypersecretion when proton pump inhibitors are stopped; increased oxyntic gastritis in H. pylori patients and the possibility of increasing the risk of gastric cancer; the possible stimulation of growth of non-gastric tumours due to hypergastrinaemia; and the possible effect of the hypo/achlorhydria on nutrient absorption, particularly iron and vitamin B12.
Because few patients with idiopathic gastro-oesophageal reflux disease/peptic ulcer disease have been treated long-term (i.e., >10 years), there is little known to address the above areas of potential concern.
Measuring Gastric PH- Heidelberg Capsule
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1930240
Can Med Assoc J. 1970 May 23; 102(10): 1087–1089.
Tubeless gastric analysis with a radiotelemetering pill (Heidelberg capsule).M. R. Andres, Jr and J. R. Bingham
http://www.phcapsule.com/
The pH Capsule is a Self-Contained pH Measuring Device. The Heidelberg pH Diagnostic System is a State-of-the-Art Diagnostic Tool for Measuring the pH Levels in the Digestive Tract. The Heidelberg pH Capsule is a Technically advanced Micro-Electronic Diagnostic Tool that can Accurately Diagnose a Patient who may have Hypochlorhydria, Hyperchlorhydria, Achlorhydria, Pyloric Insufficiency, and Heavy Mucus.
Why Stomach Acid Is Good For You – Jonathan Wright
http://www.vrp.com/articles.aspx?ProdID=art784&zTYPE=2
Why Stomach Acid is Good For You The Gray Man
By Jonathan Wright, MD, and Lane Lenard, PhD
http://www.tahoma-clinic.com/aging2.shtml
Since 1976, I’ve checked literally thousands of individuals complaining of “heartburn” and indigestion for stomach acid production using a commercially available, extremely precise, research-verified procedure. Overacidity is almost never found, especially in those over age 35. The usual findings are underacidity (from “just a little under” to no acid at all) or normal acidity, in which case the indigestion symptoms are caused by something else. The majority have underacidity (as might be expected in a no-longer-young stomach) and I advise them to take capsules containing hydrochloric acid and pepsin with each meal. The supplemental hydrochloric acid and pepsin not only relieve the symptoms but actually improve digestion.
http://www.ahha.org/AntacidsArticle.htm
Age and Antacids: A Double Whammy Against Your Body’s Optimal Health
This article was published in the March, 2007 issue of the Dr. Jonathan V. Wright’s Clinical Nutrition & Healing newsletter.
http://www.healthfreedom.net/index.php?option=com_content&task=view&id=873
Stomach Trouble: Too Little Acid? Are Antacids and acid blockers curing—or causing—stomach troubles? A fascinating new book by highly respected doctor Jonathan Wright MD that is packed with scientific citations suggests the conventional treatment for the stomach may be making things worse– and not just in the stomach.
http://www.amazon.com/Why-Stomach-Acid-Good-You/dp/0871319314/ref=ntt_at_ep_dpi_1
Why Stomach Acid is Good for You: Natural Relief from Heartburn, Indigestion, Reflux and GERD (Paperback) by Jonathan Wright
Apple Cider Vinegar
http://www.gilbertguide.com/articles/stomaching-stomach-acid-a-simple-solution/
Stomaching Stomach Acid: A Simple Solution
Unless you have been told you have an ulcer or a hiatal hernia causing your symptoms,
chances are you need to stimulate more acid secretion. One simple trick is taking a half teaspoon of organic apple cider vinegar in half a cup of water before meals.
For many of my patients, this is all that is needed to stop acid reflux.
http://www.alignlife.com/are-you-really-secreting-too-much-stomach-acid-.html
ARE YOU REALLY SECRETING TOO MUCH STOMACH ACID
When you increase the stomach acid in most cases it alleviates the problem and increases digestion. As mentioned above, the stomach acid will sterlize the gut, increase enzyme production and improve vitamin and mineral absorption.
I am aware this is the EXACT opposite management used by conventional medicine. I know it sounds a little crazy but the reality is that stomach acid decreases as you age in addition to the other factors that weaken stomach acid and in most cases we need more acid to fix the problem.
One simple test to see if you could suffer from low stomach acid, known as “hypochlorhydria”, would be to take one teaspoon of apple cider vinegar with your meals and see if you feel better. There is a protocol of taking tablets of Betain HCL (acid) that was written in the Encyclopedia of Natural Medicine and I have used if for twelve years in five different clinics around the nation with a 95% success rate.
Acid Blocker reduces Iron Absorption
http://www.ncbi.nlm.nih.gov/pubmed/7286584
Gastroenterology. 1981 Dec;81(6):1068-71.
Role of gastric acid in food iron absorption. Skikne BS, Lynch SR, Cook JD.
Radioiron absorption tests in human volunteers demonstrated a modest but significant 28% reduction in the absorption of dietary nonheme iron from a meal that was preceded by the administration of 300 mg cimetidine. More pronounced decreases of 42% and 65% were observed with 600 and 900 mg cimetidine, respectively.
PPI’s cause Malabsorption of B12
http://www.annals.org/cgi/content/abstract/120/3/211
Omeprazole Therapy Causes Malabsorption of Cyanocobalamin (Vitamin B12)
Stefan P. Marcuard; Lisa Albernaz; and Prabhaker G. Khazanie Annal of Internal Med February 1994 Volume 120 Issue 3 Pages 211-215 Conclusions: Omeprazole (Prilosec) therapy acutely decreased cyanocobalamin (B12) absorption in a dose-dependent manner.
Supplemental HCL in Achlorhydria Improves B12 Absorption
http://www.cmaj.ca/cgi/content/full/172/4/450-a
CMAJ • February 15, 2005; 172 (4). doi:10.1503/cmaj.1041424.
Cobalamin deficiency in elderly patients – Jonathan E. Prousky
Associate Dean of Clinical Education, Chief Naturopathic Medical Officer, The Canadian College of Naturopathic Medicine, Toronto, Ont.
Supplemental HCl has been shown to reduce (acidify) gastric pH in subjects with simulated hypochlorhydria.7 The method of administration has been described by several investigators.5,8,9,10
Patients usually start with one 5- to 10-grain (325- to 650-mg) capsule of betaine or glutamic acid hydrochloride with each meal; pepsin is sometimes added to these capsules to improve absorption.
Patients are instructed to increase the dosage by one 5- to 10-grain capsule with each meal, sometimes working up to 60–80 grains with every meal.
Patients are advised against this therapy if they are also receiving nonsteroidal anti-inflammatory medications or corticosteroids, if they have active peptic ulcer disease, if they have abdominal pain, or if they experience abdominal pain or burning with this treatment. Patients are also instructed to use fewer capsules with smaller meals and more capsules at larger meals.
http://www.jacn.org/cgi/content/abstract/13/6/584Journal of the American College of Nutrition, Vol 13, Issue 6 584-591, 1994 by American College of Nutrition CLINICAL TRIAL
Effect of hypochlorhydria due to omeprazole treatment or atrophic gastritis on protein-bound vitamin B12 absorption J. R. Saltzman, J. A. Kemp, B. B. Golner, M. C. Pedrosa, G. E. Dallal and R. M. Russell USDA Human Nutrition Research Center on Aging, Tufts University, Boston, MA.
Omeprazole causes protein-bound vitamin B12 malabsorption, and ingestion of an acidic drink improves protein-bound vitamin B12 absorption.
http://www.diagnose-me.com/treat/T156353.html Hydrochloric Acid (Trial)
Achlorhydria and B12 Not A Problem (?) Nonsensical medical literature
http://jama.ama-assn.org/cgi/content/summary/278/20/1659-a
Gastric Hypochlorhydria and Achlorhydria in Older Adults-Reply Aryeh Hurwitz, MD; Constance Ruhl, MD, MPH University of Kansas Medical Center Kansas City JAMA. 1997;278(20):1659-1660.
The studies by Dr Russell and colleagues have added to our appreciation that achlorhydria, resulting from either omeprazole administration or atrophic gastritis, can cause malabsorption of protein-bound vitamin B12.1 Though we did not determine absorption or levels of vitamin B12, we do not share his view that our data show one third of elderly Americans to be at risk of malabsorption of food-bound vitamin B12.
Achlorhydria http://en.wikipedia.org/wiki/Achlorhydria
H Pylori Infection Reduces Serum Ferritin
The American Journal of Gastroenterology (2001) 96, 1014–1018; Helicobacter pylori infection and serum ferritin: a population-based study among 1806 adults in Germany Gabriele Berg PhD, MPH1,2, Günter Bode PhD1, Maria Blettner PhD2, Heiner Boeing PhD, MPH3 and Hermann Brenner MD, MPH1,4
Conclusions: The decreased serum ferritin concentration among subjects infected with H. pylori might be induced by the uptake of ferritin in the stomach by H. pylori. Possible health implications of H. pylori-induced low ferritin levels warrant further investigation.
Iron Deficiency Anemai Due To H Pylori Gastritis
http://www.springerlink.com/content/jw39wenkbfp1mra0/
Refractory iron-deficiency anaemia due to silent Helicobacter pylori gastritis in children
We describe the cases of three children with chronic active Helicobacter pylori gastritis and iron-deficiency anaemia without evidence of oesophagogastrointestinal bleeding. In all cases, long-standing iron supplementation became effective only after eradication of Helicobacter pylori. Conclusion: Iron-deficiency anaemia may be due to clinically inapparent H. pylori gastritis.
Achlorhydia and Atrophic Gastritis
http://www.townsendletter.com/July2004/unseenepidemic0704.htm
The unseen epidemic: the linked syndromes of achlorhydria and atrophic gastritis
Townsend Letter for Doctors and Patients, July, 2004 by Nigel Plummer
Atrophic gastritis affects 20-30% of the adult population.
Incidence increases with age
Atrophic gastritis is highly associated with Helicobacter pylori infection.
Hypochlorhydria is probably the most common symptom of atrophic gastritis.
Gastric acid secretion does not decrease with increasing age in healthy (non atrophic gastritis) individuals.
Hypochlorhydria can result in increased risk of enteric infections, nutrient malabsorption, bacterial overgrowth and dysbiosis, and increased permeability of the intestine
Atrophic gastritis is a strong risk factor for gastric and duodenal ulcers and gastric cancer
Effects of atrophied gastric mucosa remain for months or years after eradication of H. pylori
Resolution of atrophic gastritis and symptoms depends upon:
a. elimination of H. pylori
b. treatment of residual atrophic gastritis.
Psychiatric Manifestations of B12 deficiency
http://www.ncbi.nlm.nih.gov/pubmed/15029091
Encephale. 2003 Nov-Dec;29(6):560-5.
Psychiatric manifestations of vitamin B12 deficiency: a case report] Antibodies to parietal cells were positive in the serum and antibodies to intrinsic factor were negative.
Listing of PPI’s Names
Omeprazole (Losec, Prilosec, Zegerid, ocid); Lansoprazole (Prevacid, Zoton, Inhibitol); Esomeprazole (Nexium); Pantoprazole ( Protonix, Somac, Pantoloc, Pantozol, Zurcal, Pan); Rabeprazole ( Rabecid, Aciphex, Pariet, Rabeloc)
Dr Kuipers – Expert on PPI’s, Atrophic Gastritis
PPI’s accelerate Atrophic Gastritis Caused by H Pylori
http://www.ncbi.nlm.nih.gov/pubmed/8598839
N Engl J Med. 1996 Apr 18;334(16):1018-22.
Atrophic gastritis and Helicobacter pylori infection in patients with reflux esophagitis treated with omeprazole or fundoplication. Kuipers EJ et al.
BACKGROUND. Helicobacter pylori infection plays an important part in the development of atrophic gastritis and intestinal metaplasia, conditions that predispose patients gastric cancer. Profound suppression of gastric acid is associated with increased severity of gastritis caused by H. pylori, but it is not known whether acid suppression increases the risk of atrophic gastritis. CONCLUSIONS. Patients with reflux esophagitis and H. pylori infection who are treated with omeprazole are at increased risk of atrophic gastritis.
Recommendation: Eradicate H Pylori in GERD pts on Long term PPI’s
http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pubmed&pubmedid=14684569
Gut. 2004 January; 53(1): 12–20.
Cure of Helicobacter pylori infection in patients with reflux oesophagitis treated with long term omeprazole reverses gastritis without exacerbation of reflux disease: results of a randomised controlled trial. E J Kuipers et al.
Conclusions: Most H pylori positive GORD patients have a corpus predominant pangastritis during omeprazole maintenance therapy. Eradication of H pylori eliminates gastric mucosal inflammation and induces regression of corpus glandular atrophy. H pylori eradication did not worsen reflux disease or lead to a need for increased omeprazole maintenance dose. We therefore recommend eradication of H pylori in GORD patients receiving long term acid suppression.
http://www.ncbi.nlm.nih.gov/pubmed/16508317
Gerontology. 2006;52(2):99-106.
Effect of Helicobacter pylori eradication on the outcome of reflux esophagitis and chronic gastritis in the elderly. A randomized, multicenter, eight-month study. Pilotto A, Perri F, Leandro G, Franceschi M; Aging and Acid-Related Disease Study Group.
CONCLUSION: The eradication of H. pylori infection does not affect the clinical outcome of esophagitis, while it improves chronic gastritis and its activity in elderly patients on short- and long-term treatment with PPIs. These findings suggest that H. pylori infection should be eradicated in elderly patients with esophagitis who need maintenance treatment with PPI.
Triple Therapy Protocol for Eradication of H Pylori
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1140724
MedGenMed. 2004; 6(1): 19. 2004 February 18.
Eradication of Helicobacter pylori: A Clinical Update – Marco Romano, MD and Antonio Cuomo, MD
First-line therapy should be a PPI-based triple therapy employing a PPI (standard dose twice daily) combined with clarithromycin (500 mg twice daily) and amoxicillin (1 g twice daily), for a minimum of 7 days.
Triple Therapy for H Pylori Eradication Cures Peptic Ulcer Disease
http://en.wikipedia.org/wiki/Helicobacter_pylori
Once H. pylori is detected in patients with a peptic ulcer, the normal procedure is to eradicate it and allow the ulcer to heal. The standard first-line therapy is a one week triple therapy consisting of the antibiotic clarithromycin, and a proton pump inhibitor such as omeprazole.[40] Variations of the triple therapy have been developed over the years, such as using a different proton pump inhibitor, as with pantoprazole or rabeprazole, or replacing amoxicillin with metronidazole for people who are allergic to penicillin.[41] Such a therapy has revolutionized the treatment of peptic ulcers and has made a cure to the disease possible; previously the only option was symptom control using antacids, H2-antagonists or proton pump inhibitors alone.[42][43] While H. pylori has been disappearing from the stomach of humans, the incidence of the related disorders acid reflux disease, Barrett’s esophagus, and esophageal cancer have been rising dramatically.[51] See also: Timeline of peptic ulcer disease and Helicobacter pylori
Helicobacter pylori (H.pylori for short) was first discovered in the stomachs of patients with gastritis & stomach ulcers nearly 25 years ago by Dr Barry J. Marshall and Dr J. Robin Warren of Perth, Western Australia. Marshall & Warren literally “re-wrote” the text-books with reference to what causes gastritis & gastric ulcers. In recognition of their very important discovery, they were Awarded the 2005 Nobel Prize for Medicine & Physiology.
German scientists found spiral-shaped bacteria in the lining of the human stomach in 1875, but they were unable to culture it and the results were eventually forgotten.[51] The Italian researcher Giulio Bizzozero described similarly shaped bacteria living in the acidic environment of the stomach of dogs in 1893.[65] Professor Walery Jaworski of the Jagiellonian University in Kraków investigated sediments of gastric washings obtained from humans in 1899. Among some rod-like bacteria, he also found bacteria with a characteristic spiral shape, which he called Vibrio rugula. He was the first to suggest a possible role of this organism in the pathogenesis of gastric diseases. This work was included in the Handbook of Gastric Diseases, but it had little impact as it was written in Polish.[66] Several small studies conducted in the early 1900s demonstrated the presence of curved rods in the stomach of many patients with peptic ulcers and stomach cancer.[67] However interest in the bacteria waned when an American study published in 1954 failed to observe the bacteria in 1180 stomach biopsies.[68]
Interest in understanding the role of bacteria in stomach diseases was rekindled in the 1970s with the visualization of bacteria in the stomach of gastric ulcer patients.[69] The bacterium had also been observed in 1979 by Australian pathologist Robin Warren, who did further research on it with Australian physician Barry Marshall beginning in 1981. After numerous unsuccessful attempts at culturing the bacteria from the stomach, they finally succeeded in visualizing colonies in 1982 when they unintentionally left their Petri dishes incubating for 5 days over the Easter weekend. In their original paper, Warren and Marshall contended that most stomach ulcers and gastritis were caused by infection by this bacterium and not by stress or spicy food as had been assumed before.[70]
Although there was some skepticism initially, within several years, numerous research groups verified the association of H. pylori with gastritis and to a lesser extent ulcers.[71] To demonstrate that H. pylori caused gastritis and was not merely a bystander, Marshall drank a beaker of H. pylori. He became ill several days later with nausea and vomiting. An endoscopy ten days after inoculation revealed signs of gastritis and the presence of H. pylori. These results suggested that H. pylori was the causative agent of gastritis. Marshall and Warren went on to show that antibiotics are effective in the treatment of many cases of gastritis. In 1987 the Sydney gastroenterologist Thomas Borody invented the first triple therapy for the treatment of duodenal ulcers.[72] In 1994, the National Institutes of Health (USA) published an opinion stating that most recurrent duodenal and gastric ulcers were caused by H. pylori and recommended that
http://en.wikipedia.org/wiki/Timeline_of_peptic_ulcer_disease_and_Helicobacter_pylori
Testing for Helicobacter Pylori
Quest- Helicobacter pylori Urea Breath Test, Infra-red (UBiT ® 14839 CPT Code(s): 83013
HELICOBACTER PYLORI IGG ANTIBODY (REFL) 31314 CPT Code(s): 86677
H Pylori Eradication: Guidelines on WHO to Treat
Test and Treat under age of 45
http://www.ncbi.nlm.nih.gov/pubmed/11860399
Aliment Pharmacol Ther. 2002 Feb;16(2):167-80.
Current concepts in the management of Helicobacter pylori infection–the Maastricht 2-2000 Consensus Report. Malfertheiner P, Mégraud F, O’Morain C, Hungin AP, Jones R, Axon A, Graham DY, Tytgat G; European Helicobacter Pylori Study Group (EHPSG).
A “test and treat” approach is recommended in adult patients under the age of 45 years (the age cut-off may vary locally) presenting in primary care with persistent dyspepsia, having excluded those with predominantly gastro-oesophageal reflux disease symptoms, non-steroidal anti-inflammatory drug users and those with alarm symptoms.
Diagnosis of infection should be by urea breath test or stool antigen test. As in the previous guidelines, the eradication of H. pylori is strongly recommended in all patients with peptic ulcer, including those with complications, in those with low-grade gastric mucosa-associated lymphoid tissue lymphoma, in those with atrophic gastritis and following gastric cancer resection.
Successful eradication should always be confirmed by urea breath test or an endoscopy-based test if endoscopy is clinically indicated. Stool antigen test is the alternative if urea breath test is not available.
The European Helicobacter Pylori Study Group published the Maastricht 2-2000 Consensus Report, suggesting a test-and-treat strategy for H. pylori in young patients without atypical symptoms. This strategy advocates the use of non-invasive testing to evaluate for H. pylori and simply treating if found, even in the absence of ulcer disease documented on endoscopy.[46]
Discovery of H Pylori- Marshall Nobel Prize
http://nobelprize.org/nobel_prizes/medicine/laureates/2005/index.html
The Nobel Prize in Physiology or Medicine 2005 for their discovery of the bacterium Helicobacter pylori and its role in gastritis and peptic ulcer disease”
Breathe Test for H Pylori
http://www.ncbi.nlm.nih.gov/pubmed/2593958
Med J Aust. 1989 Oct 16;151(8):435-9.
The 14C-urea breath-test for the detection of gastric Campylobacter pylori infection.
Surveyor I, Goodwin CS, Mullan BP, Geelhoed E, Warren JR, Murray RN, Waters TE, Sanderson CR.
Royal Perth Hospital, WA.
We consider that the 14C-urea breath-test has an important role in the noninvasive confirmation of gastric infection with H. pylori and in the follow-up of patients after treatment.
http://www.ncbi.nlm.nih.gov/pubmed/10882957
Gastrointest Endosc. 2000 Jul;52(1):20-6
Noninvasive tests as a substitute for histology in the diagnosis of Helicobacter pylori infection.
Hahn M, Fennerty MB, Corless CL, Magaret N, Lieberman DA, Faigel DO.
Division of Gastroenterology, Portland VA Medical Center and Oregon Health Sciences University, OR 97201, USA.
CONCLUSIONS: Whole blood or serum antibody testing is a rapid, accurate, and cost-effective means for establishing H pylori status in rapid urease test-negative patients. Whole blood or serology rapid antibody testing should substitute for histology when the patient has not been previously treated for H pylori.
Eradication of H Pylori in GERD
http://gut.bmj.com/cgi/eletters/53/1/5
H pylori infection and reflux oesophagitis – Jannis Kountouras, we suggest that Hp eradication leads to better control of GORD symptoms and improves oesophagitis.
PPI’s and Gastritis
http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2266058
J Clin Biochem Nutr. 2008 March; 42(2): 71–75.
Proton Pump Inhibitors and Gastritis- Masayuki Suzuki,1* Hidekazu Suzuki,2 and Toshifumi Hibi2
Use of Probiotics with PPI’s and Triple Therapy for H Pylori ERadication
http://www.ingentaconnect.com/content/bsc/hel/2008/00000013/00000004/art00006
The Effects of Probiotics on PPI-Triple Therapy for Helicobacter pylori Eradication
Authors: Kim, Mi Na1; Kim, Nayoung; Lee, Sang Hyup2; Park, Young Soo; Hwang, Jin-Hyeok; Kim,
The addition of Will yogurt to triple therapy did not reduce the side-effects of triple therapy. But it increased the H. pylori eradication rate by PP analysis, encouraging more research in this field.
PPI’s Update American Acad Fam Physicians-2002
Triple Therapy Protocol
http://www.aafp.org/afp/20020715/273.html
Proton Pump Inhibitors: An Update 2002 by the American Academy of Family Physicians.
BRUCE T. VANDERHOFF, M.D., and RUNDSARAH M. TAHBOUB, M.D. Grant Medical Center, Columbus, Ohio
Helicobacter pylori eradication for reduction of duodenal ulcer recurrence
Dosage: Triple therapy: omeprazole, 20 mg, clarithromycin, 500 mg, and amoxicillin, 1,000 mg, each taken twice daily. Dual therapy: omeprazole, 40 mg daily, and clarithromycin, 500 mg, each three times daily Duration of Treatment, Triple therapy: 10 days, plus 18 days of omeprazole therapy if an ulcer is present at initiation of treatment. Dual therapy: 14 days, plus 14 days of omeprazole therapy at 20 mg daily if an ulcer is present at initiation of treatment
http://www.ncbi.nlm.nih.gov/pubmed/9679031
Gastroenterology. 1998 Aug;115(2):268-74.
Serum ferritin, hemoglobin, and Helicobacter pylori infection: a seroepidemiologic survey comprising 2794 Danish adults. Milman N, Rosenstock S, Andersen L, Jørgensen T, Bonnevie O.
Department of Medicine, Naestved Hospital, Naestved, Denmark. CONCLUSIONS: Serum ferritin levels are reduced in people with increased IgG antibodies to H. pylori. H. pylori infection affects iron metabolism in humans.
http://www.ncbi.nlm.nih.gov/pubmed/10577329
Ann Intern Med. 1999 Nov 2;131(9):668-72.
Reversal of iron deficiency anemia after Helicobacter pylori eradication in patients with asymptomatic gastritis. Annibale B, Marignani M, Monarca B, Antonelli G, Marcheggiano A, Martino G, Mandelli F, Caprilli R, Delle Fave G. University La Sapienza, Rome, Italy.
BACKGROUND: Iron deficiency anemia is the most common form of anemia worldwide. Recent studies have suggested an association between Helicobacter pylori infection and iron deficiency. CONCLUSIONS: Cure of H. pylori infection is associated with reversal of iron dependence and recovery from iron deficiency anemia.
http://www.wjgnet.com/1007-9327/13/5380.asp
World J Gastroenterol 2007 October 28; 13(40): 5380-5383 Effects of H pylori therapy on erythrocytic and iron parameters in iron deficiency anemia patients with H pylori-positive chronic gastristis Lun-Hua Chen, He-Sheng Luo
http://www.ncbi.nlm.nih.gov/pubmed/17211708
Dig Dis Sci. 2007 Feb;52(2):405-10. Epub 2007 Jan 9.
Serum ferritin, vitamin B(12), folate, and zinc levels in children infected with Helicobacter pylori. Akcam M, Ozdem S, Yilmaz A, Gultekin M, Artan R. findings of the present study suggest that H. pylori infection has a negative effect on serum ferritin and vitamin B(12) levels in children.
http://www.ncbi.nlm.nih.gov/pubmed/12827006
J Pediatr Gastroenterol Nutr. 2003 Jul;37(1):53-62. Correlation between Helicobacter pylori infection and vitamin C levels in whole blood, plasma, and gastric juice, and the pH of gastric juice in Korean children. Park JH, Kim SY, Kim DW, Lee WG, Rhee KH, Youn HS.
Department of Pediatrics
CONCLUSIONS: The data demonstrate that vitamin C levels in whole blood, plasma, and gastric juice and the gastric juice pH in Korean children are closely related to the severity of H. pylori infection and the histologic changes in the stomach. These data suggest that vitamin C may play a role in determining infection and progression, and vitamin C supplementation may be an important axis for the management of H. pylori infection in children.
http://www.johnshopkinshealthalerts.com/reports/digestive_health/869-1.html
Digestive Health Special Report – The H. Pylori Story
For most of the 20th century, peptic ulcers were rarely cured. The reigning theory said that ulcers resulted from psychological stress and dietary factors (such as spicy foods), and patients were routinely hospitalized, told to get bed rest, and instructed to eat a bland diet. Doctors later added excess stomach acid to the list of potential causes for peptic ulcers, and patients typically received long-term therapy with medications that reduced stomach acid or blocked its production. Even with these treatments, however, ulcers were often a recurring, life-long condition.
Yet, as far back as 1886, researchers had documented a possible association between ulcers and spiral bacteria in the lining of the human stomach. Mainstream medicine dismissed this finding, however, because it was believed that no bacteria could live in the acidic environment of the stomach. Then, almost a century later, two Australian researchers rediscovered this bacterium and radically changed — and improved — the way peptic ulcers are diagnosed and treated. Meet Drs. Warren and Marshall In 1981, Robin Warren, M.D., a pathologist at the Royal Perth Hospital in Western Australia, discovered numerous bacteria living in tissue taken during a stomach biopsy. Over time, he began to notice a pattern in stomach biopsies: The spiral bacteria that he observed always accompanied changes in the stomach lining caused by gastritis (an inflammation of the stomach lining). Generally, his colleagues dismissed his discovery.
Later that year, Barry Marshall, M.D., joined Dr. Warren in his research, and together they verified the link between the spiral bacterium — later termed Helicobacter pylori — and the presence of peptic ulcers.
Helicobacter pylori infection and dermatologic diseases
European Journal of Dermatology. Volume 19, Numéro 5, 431-44, September-October 2009, Review article Ana C Hernando-Harder, Nina Booken, Sergij Goerdt, Manfred V Singer, Hermann Harder
Summary : Recent evidence suggests that Helicobacter pylori infections play a role in the pathogenesis of a variety of skin diseases. The best evidence for such a link is found for two diseases: chronic urticaria and immune thrombocytopenic purpura. Other diseases that have a purported, but not yet proven link to H. pylori are: cutaneous pruritus, Behçet’s disease, nodular prurigo and lichen planus.
http://supplementwatch.blogspot.com/2009/08/mastic.html
Mastic – Overview
Mastic is a resin, or gum, that is extracted from a tree from the Mediterranean or Middle Eastern regions. Long used as a chewing gum and a traditional medicine, mastic resin also has been developed for use in numerous industrial applications (Milov et al., 1998). Preliminary clinical evidence has confirmed mastic resins use to be useful in the treatment of ulcer. Mastic has been further shown to exhibit antibacterial activity against Helicobacter pylori, explaining its efficacy in ulcers. Mastic has also shown antibacterial, antiplaque and antigingival activity in the saliva and on the teeth (Takahashi et al., 1998).
One gram daily is used for treating ulcers and gastrointestinal discomfort. Mastic is not known to product any side effects, and is thought to be safe (Al-Habbal et al., 1984).
Al-Habbal MJ, Al-Habbal Z, Huwez FU. A double-blind controlled clinical trial of mastic and placebo in the treatment of duodenal ulcer. Clin Exp Pharmacol Physiol. 1984 Sep-Oct;11(5):541-4.
Huwez FU, Al-Habbal MJ. Mastic in treatment of benign gastric ulcers. Gastroenterol Jpn. 1986 Jun;21(3):273-4.
http://content.nejm.org/cgi/content/extract/339/26/1946
Volume 339:1946 December 24, 1998 Number 26
Mastic Gum Kills Helicobacter pylori
To the Editor: Even low doses of mastic gum — 1 g per day for two weeks — can cure peptic ulcers very rapidly, but the mechanism responsible has not been clear. We have found that mastic is active against Helicobacter pylori, which could explain its therapeutic effect in patients with peptic ulcers. Mastic is a resinous exudate obtained from the stem and the main leaves of Pistacia lentiscus. It is used as a food ingredient in the Mediterranean region. Clinically, mastic has been effective in the treatment of benign gastric ulcers1 and duodenal ulcers.2 In rats, mastic showed cytoprotective .
http://www.healthandwellnessfoundation.org/monographs/helicobacter_pylori.pdf
Helicobacter pylori Eradication: Are there Alternatives to Antibiotics? Alan R. Gaby, MD
http://www.koreamed.org/SearchBasic.php?DT=1&RID=474823
Korean J Gastroenterol. 2003 Apr;41(4):277-283. Korean.
The Effect of Mastic Gum on Helicobacter pylori-infected Gastritis. Roe IH, Nam SW, Myung NH, Kim JT, Shin JH. , Korea.
BACKGROUND/AIMS: Mastic, a natural resin obtained from the Pistacia lentiscus tree, has been reported to have an antimicrobial activity against Helicobacter pylori (H. pylori). We investigated the effects of mastic containing chewing gum on the subjects with H. pylori-infected gastritis. CONCLUSIONS: Mastic gum has a beneficial effect on H. pylori-infected gastritis, and can be considered as one of novel treatments.
http://en.wikipedia.org/wiki/Pistacia_lentiscus
Mastic resin is a relatively expensive kind of spice, that has been used, principally, as a chewing gum, for at least 2,400 years[6]. The flavour can be described as a strong slightly smoky, resiny aroma and can be an acquired taste. Some scholars identify the bakha בכא mentioned in the Bible – as in the Valley of Baca (Hebrew: עמק הבכא) of Psalm 84 – with the mastic plant. The word bakha appears to be derived from the Hebrew word for crying or weeping, and is thought to refer to the “tears” of resin secreted by the mastic plant, along with a sad weeping noise which occurs when the plant is walked on and branches are broken. The Valley of Baca is thought to be a valley near Jerusalem that was covered with low mastic shrubbery, much like some hillsides in northern Israel today.
http://aac.asm.org/cgi/content/full/51/2/551
Antimicrobial Agents and Chemotherapy, February 2007, p. 551-559, Vol. 51, No. 2
0066-4804/07/
In Vitro and In Vivo Activities of Chios Mastic Gum Extracts and Constituents against Helicobacter pylori Sotirios Paraschos,1 Prokopios Magiatis,1 Sofia Mitakou,1* Kalliopi Petraki,2 Antonios Kalliaropoulos,2 Petros Maragkoudakis,2 Andreas Mentis,2 Dionyssios Sgouras,2* and Alexios-Leandros Skaltsounis1
http://books.google.com/books?hl=en&lr=&id=KDxUfc-rEs8C&oi=fnd&pg=
PA159&ots=-uSsoF3d7v&sig=rUuePxYsCb3Dxu-7AqHdVPdVwcI#v=onepage&q=&f=false
gASTRO-iNTESTINAL rEFLUX dISEASE BY mARK hYMAN md
http://www.ultrawellness.com/blog/heart-burn-and-acid-reflux
3 simple steps to eliminate heart burn and acid reflux
MARK HYMAN
http://www.youtube.com/watch?v=ORY1cUB_k6M
3 Simple Steps to Eliminate Heartburn and Acid Reflux by
Mark Hyman MD Do you suffer from acid reflux or heartburn? If so, you know how miserable that burning sensation in your gut can be. In this weeks UltraWellness blog, Dr. Mark Hyman outlines a 3-step program.
Jeffrey Dach MD
7450 Griffin Road Suite 190
Davie, Florida 33314
954-792-4663
http://www.jeffreydach.com/
http://www.drdach.com/
http://www.naturalmedicine101.com/
http://www.truemedmd.com/
http://www.bioidenticalhormones101.com/
Disclaimer click here: http://www.drdach.com/wst_page20.html
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this article: http://wp.me/P3gFbV-xO
http://jeffreydach.com/2009/09/14/heartburn-and-acid-blockers-by-jeffrey-dach-md.aspx
Copyright (c) 2009-2013 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.








{kind=link}
{kind=link}
Hair Loss From Low Stomach Acid, by Jeffrey Dach MD July 17, 2013 at 8:12 AM
[…] Heartburn GE Reflux (GERD) and Acid Blocker Drugs […]
A Neurosurgeon with a Painful Arm, Myositis from Statin and PPI Drugs January 28, 2014 at 7:24 AM
[…] GERD, GE Reflux and Heartburn […]
Homepage March 3, 2014 at 10:41 PM
… [Trackback]
[…] Find More Informations here: jeffreydachmd.com/heartburn-ge-reflux-gerd-and-acid-blocker-drugs/ […]
Rosacea and Low Stomach Acid by Jeffrey Dach MD - Jeffrey Dach MD October 1, 2014 at 10:09 AM
[…] Acid Blocker Drugs […]