954-792-4663
 Clomid For Men with Low Testosterone, Part Two
Clomid For Men with Low Testosterone, Part Twoby Jeffrey Dach MD
This article is Part Two of a series,
Click Here for Part One.
For Part Three, Click Here
Left Image: James Stewart, Screenshot from the original 1958 theatrical trailer for the film Vertigo courtesy of Wikimedia commons.A Case Report
Jim, a 34 year old accountant from Britain, arrived in my office complaining of low testosterone symptoms of low libido, erectile dysfunction, chronic fatigue, and mood disorder. A previous blood panel revealed a low testosterone level (242 ng/dl), low LH (1.6 iu/L) and FSH (1.7 iu/L).
Jim had been married 5 years, and together with his wife, had a 2 year old daughter. For younger males who wish to expand their families, testosterone replacement is not advisable, since this interferes with fertility.
In the past, Jim had seen a number of doctors including an internist, a hematologist, and an endocrinologist. One gave Jim a trial of Clomiphene, Clomid, 25 mg a day for 3 weeks, and a repeat lab panel showed no increase in either testosterone or LH/FSH levels. This is Clomid Stimulation Test failure, indicating Clomid is not a suitable treatment. Jim’s previous doctor gave up in frustration, and Jim wanted to know, “What’s next?”.
Next, most endocrinologists will order an MRI scan of the pituitary gland and brain to rule out a pituitary lesion. This was done and the MRI scan was normal.
The Clomid Stimulation Test is one of the best methods for evaluating hypothalamic function (8). The failed Clomid Stimulation Test is virtually diagnostic of hypothalamic dysfunction, representing a complex condition with dysfunction of all hormonal systems in the body.(8) There is typically a blunted response to ACTH, low adrenal function, and a paradoxically low TSH in spite of low thyroid function, all associated with chronic fatigue.
Jim told his story of many years of markedly reduced libido, anxiety, panic attacks, and chronic fatigue unrelieved by sleep. Jim’s symptoms started about 10 years ago in his late 20’s during which time he was living in London, going to school during the week, and on weekends, “clubbing” with his friends which meant recreational drug use with Ecstasy (MDMA), virtually every weekend for five years.

Left image: Dancing at a nightclub (“clubbing”). 2006. Clubbing on Ecstasy Courtesy of Wikimedia Commons
Ecstasy (MDMA) is a chemically modified synthetic amphetamine drug that floods the brain with serotonin and dopamine, the two major neurotransmitters. This produces an intensely pleasurable effect, with 800% increase in cortisol levels on the dance floor while “clubbing” on Ecstasy.(18) Long term MDMA use shows damage to the serotonergic terminal axonal nerves in the hypothalamus. (14-16) These important nerve axons are responsible for pituitary signalling which controls endocrine function. This damage may or may not be reversible.(5,12-20)
Animal studies show that hypothalamic gonadotropin levels are suppressed in the context of low testosterone suggesting that the hypothalamic neurosecretory system “is a primary target” of inhibition by MDMA usage.(24)

Left image : Ecstasy (MDMA) Tablets, Courtesy of the DEA and WIkimedia Commons.
Examination of brain photomicrographs of monkeys given MDMA reveals loss of serotonergic axons in the hypothalamus, with some abnormalities persisting for seven years. (25)
Years of Weekend “Clubbing” and “Raves” with the recreational use of Ecstasy has created an entire generation, called Generation E.(12-20). Many of these Post-MDMA, post-Ecstasy members of Generation E are now suffering from low testosterone and other symptoms of hypothalmic dysfunction with chronic fatigue and fibromyalgia. They may find it difficult to find a physician who has the knowledge and experience to help them.
As noted by Michael H. Baumann in the January 2007 issue of Psychopharmacology (20), many studies have examined long term use of SSRI antidepressants such as Prozac, Paxil, Zoloft, Celexa, Effexor, paroxetine, sertraline etc, and have suggested that hypothalamic damage may be induced by SSRIs which may mimic that of MDMA(20).
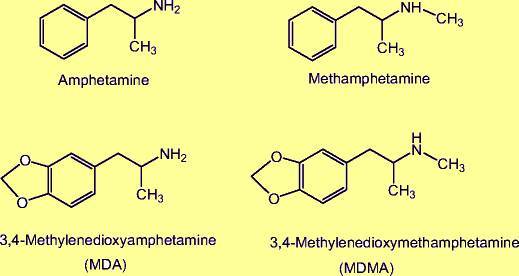 Upper image: Chemical structure of MDMA, Courtesy of Michael H. Baumann in Psychopharmacology (Berl). 2007 January; 189(4): 407–424.
Upper image: Chemical structure of MDMA, Courtesy of Michael H. Baumann in Psychopharmacology (Berl). 2007 January; 189(4): 407–424.
The drug, Ecstasy (MDMA) has been described by some as “a turbo SSRI “. (13) It is clear that MDMA has more potent immediate effects and produces long term adverse effects than SSRI antidepressants. Nonetheless, long term SSRI antidepressant use can potentially induce the same neuronal defects and chronic brain changes as those found with MDMA usage.(20) The reality is that many drugs cause hypothalamic dysfunction, including opiates, alcohol, anti-psychotics, and even inhaled or topical corticosteroids. There are many others.(21) (8)
In my office practice, we will frequently see patients on multiple psychoactive drugs prescribed by the primary care physician, internist or psychiatrist. This is a perfect example of an abusive medical practice that should be halted, and reveals a medical system gone wrong.
Many of these unfortunate victims are on combinations of drugs such as SSRI antidepressants, amphetamines (Vyvanse ,lisdexamfetamine, Adderal, Ritalin) and Benzodiazapines (Xanax, Klonopin) and Narcotics such as Oxycontin and Vicodin, etc. Some are also chronic alcohol abusers. These patients arrive at my door with a form of “Burn Out”, and drug-induced hypothalamic dysfunction characterized by chronic fatigue unrelieved by sleep. Recovery requires a gradually tapering of the drug dosage to “wean off” the psycho-active drug in order to min imize withdrawal effects. In some cases, a drug rehabilitation facility is required during the drug withdrawal phase.
Jim’s hormonal defects are more complicated than isolated low testosterone and require a treatment program as described by Jacob Teitelbaum MD (22) and Kent Holtorf MD (1-4) in their excellent books and articles covering chronic fatigue and hypothalamic dysfunction.(1-4, 22)
Dr Holtorf’s articles on hypothalamic dysfunction and chronic fatigue discuss the use low dose cortisol, usually given in doses less than 15 mg per day. In addition, Florinef, Fludrocortisone, 50 mcg, a day may be used.(1-2) A widely used nutritional supplement program for adrenal fatigue is described by Chris Miletis in the 2005 Townsend Letter (3) . This program includes Vitamin C, Pantethine (B5) and adaptogenic herbs.(3)
Endocrinologists commonly use the ACTH stimulation test to diagnose adrenal insufficiency. The ACTH stimulaton test is limited and does not evaluate the HPA axis. A better testing choice is the Metyrapone test. Unlike ACTH which requires an injection, the metyrapone drug can be given PO (orally). The metyrapone test is superior to the ACTH stimulation test because evaluates both hypothalamic and adrenal function.(4) However, in my opinion, the Clomid stimulation test is by far the best test for evaluating hypothalamic function. In agreement is Eugene Shippen MD in his comment posted here (8).
A paradoxically low TSH level accompanied by low thyroid hormone levels (Free T3 levels less than 270 ) may indicate low thyroid function from hypothalamic dysfunction.
(1-2)
The low testosterone level can be successfully treated with an LH analog called HCG (human chorionic gonadotropin) readily available at most pharmacies. HCG stimulates testicular production of testosterone without impairing fertility, and is therefore a preferred treatment in the younger age group.
Shortly after starting the HCG injections, Jim reported an immediate improvement in mood, energy and libido. Repeat labs showed a rising testosterone level of 687 ng/dl. Jim’s treatment program also included 15 mg hydrocortisone and 50 mcg Florinef daily. He was also given a small dosage of natural thyroid , a half grain tablet daily. Additional treatment protocols were also given as outlined by Dr. Jacob Teitelbaum in his books and articles (22).
Jim had hypothalamic damage from MDMA drug use which caused his low hormone levels and chronic fatigue.
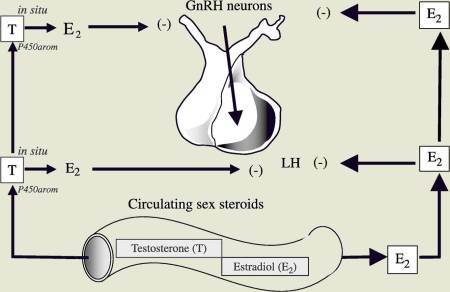 Image left: Pituitary feedback control of LH, FSH and Testosterone from Estrogen (E2). Diagram is courtesy of Dr Rochira , Eur J Endocrinol. 2006 Oct;155(4):513-22.(1)
Image left: Pituitary feedback control of LH, FSH and Testosterone from Estrogen (E2). Diagram is courtesy of Dr Rochira , Eur J Endocrinol. 2006 Oct;155(4):513-22.(1)
Normally, the hypothalamus produces gonadotropin releasing hormone (GnRH), which in turn stimulates pituitary production of LH and FSH (leutinizing hormone and follicle stimulating hormone). LH and FSH then travel to the testicle to stimulate testosterone(LH) and sperm production (FSH).
Chronic recreational drug use with Ecstasy. also called MDMA, damages Hypothalamic GNRH neurons (see above diagram upper center ).(14-16) With hypothalamic damage and dysfunction, there is absent or severely reduced GnRH release, and no stimulation for pituitary release of LH and FSH. Jim’s treatment is HCG, an LH analog which stimulates testosterone production at the level of the end organ.
Articles with related interest:
This article is Part Two of a series, Click Here for Part One.
For Part Three, Click Here
Low Testosterone From Pain Pills by Jeffrey Dach MD
Dr John Crisler on HCG for Symptoms of Low Testosterone
Low Testosterone Diagnosis and Treatment by Jeffrey Dach MD
More articles on Low Testosterone, Diagnosis and Treatment
Click Here for excellent discussion of pathophysiology of hypothalamic pituitary axis.
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
www.jeffreydach.com
www.drdach.com
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Links and References
Hypothalamic Dysfunction- chronic fatigue, low T, Adrenal fatigue, Low thyroid
Holtorf, Kent. “Diagnosis and Treatment of Hypothalamic-Pituitary-Adrenal (HPA) Axis Dysfunction in Patients with Chronic Fatigue Syndrome (CFS) and Fibromyalgia (FM).” JOURNAL OF CHRONIC FATIGUE SYNDROME 14.3 (2008).
A therapeutic trial of 5-15 mg of timed-released cortisol per day. Patients were also given fludrocortisone if they had signs of neurally mediated hypotension. Fludrocortisone is available in 0.1 mg tablets. Florinef. Usual starting dose 50 mcg (half tab) The current evidence supports the use of physiologic doses of cortisol as an appropriate component of a multi-system treatment protocol for CFS and FM, and a therapeutic trial of cortisol should be considered in the majority of these patients, especially those with signs or symptoms consistent with adrenal dysfunction, low blood pressure and/or serum levels that are low or in the low normal range.
—————
2) Treating_Chronic_Fatigue_Syndrome_Kent_Holtorf_Womens_Health
NOV/DEC 2008 • HEALTHY AGING • WWW .ADVANCEWEB.COM/HEALTHYAGING
Treating chronic fatigue syndrome and Fibromyalgia BY KENT HOLTORF, MD
An overwhelming amount of peer-reviewed medical literature documents pituitary and hypothalamic dysfunction in CFS and FM patients. As a result, patients often have multiple hormonal deficiencies 4-21, including thyroid, growth hormone and cortisol. Instead of T4 normally converting intracellularly to the active T3 in peripheral tissue, T4 is preferentially converted to reverse T3. Therefore, increasing levels of rT3 and diminishing levels of T3 are indicators of low tissue thyroid effect. Free T3 and rT3 tests can be ordered at most major clinical laboratories. A free T3/rT3 ratio that’s less than 2 pg/ng is consistent with low tissue thyroid activity.
——————
3) http://www.encognitive.com/files/The Naturopathic Approach to Adrenal Dysfunction.pdf
The Naturopathic Approach to Adrenal Dysfunction by Jason Barker, ND and Chris Meletis, ND Townsend Letter Feb March 2005
Metyrapone Test
4) www.ncbi.nlm.nih.gov/pubmed/8013141
Overnight Metyrapone Test – Clin Endocrinol (Oxf). 1994 May;40(5):603-9.
The overnight single-dose metyrapone test is a simple and reliable index of the hypothalamic-pituitary-adrenal axis. Fiad TM, Kirby JM, Cunningham SK, McKenna TJ. Source Department of Endocrinology and Diabetes Mellitus, St Vincent’s Hospital, Dublin, Ireland.
Abstract OBJECTIVE:
The ACTH stimulation test examines adrenal responsiveness but may not examine the entire hypothalamic-pituitary-adrenal (HPA) axis and requires parenteral administration. The cortisol response to hypoglycaemia provides an index of activity of the entire HPA axis but is demanding for patients and medical staff. The aim of the present study was to examine the performance of the overnight single-dose metyrapone test as it provides a simple alternative test for HPA axis function.
DESIGN: Audit of the overnight metyrapone test performed in one centre between 1979 and 1991.
PATIENTS: Three hundred and ninety-eight patients underwent 576 tests. Comparisons between the responses to metyrapone and the ACTH stimulation test and of the responses to metyrapone and insulin induced hypoglycaemia test were possible in 87 and 17 patients respectively.
MEASUREMENTS: Following the midnight administration of metyrapone tablets, 30 mg/kg orally, blood samples were obtained between 0800 and 0930 h for radioimmunoassay of both 11-deoxycortisol and cortisol.
RESULTS: Five hundred and seventy-six metyrapone tests were performed on 398 patients with no serious side-effects encountered.
Adrenal insufficiency was diagnosed in 105 patients.
Of these, 18 had a primary adrenal disorder and 87 had a disorder of the hypothalamic-pituitary unit.
One hundred per cent concordance between the metyrapone, the ACTH and the hypoglycaemia test was seen in patients with primary adrenal insufficiency.
CONCLUSION: Since the metyrapone test gives similar information about hypothalamic-pituitary axis function as does the hypoglycaemia test, we recommend the use of the overnight metyrapone test as a safe, simple and reliable index of the hypothalamic-pituitary axis integrity. The ACTH stimulation test should not be used for patients suspected of having secondary adrenal insufficiency.
————————————————-
5) www.ncbi.nlm.nih.gov/pubmed/9629295
Ann NY Acad Sci. 1998 May 1;840:684-97.
Evidence for and pathophysiologic implications of hypothalamic-pituitary-adrenal axis dysregulation in fibromyalgia and chronic fatigue syndrome. Demitrack MA, Crofford LJ. Source Lilly Research Laboratories, Lilly Corporate Center, Indianapolis, Indiana 46285, USA.
Abstract Chronic fatigue syndrome (CFS) is characterized by profound fatigue and an array of diffuse somatic symptoms. Our group has established that impaired activation of the hypothalamic-pituitary-adrenal (HPA) axis is an essential neuroendocrine feature of this condition. The relevance of this finding to the pathophysiology of CFS is supported by the observation that the onset and course of this illness is excerbated by physical and emotional stressors. It is also notable that this HPA dysregulation differs from that seen in melancholic depression, but shares features with other clinical syndromes (e.g., fibromyalgia). How the HPA axis dysfunction develops is unclear, though recent work suggests disturbances in serotonergic neurotransmission and alterations in the activity of AVP, an important co-secretagogue that, along with CRH, influences HPA axis function. In order to provide a more refined view of the nature of the HPA disturbance in patients with CFS, we have studied the detailed, pulsatile characteristics of the HPA axis in a group of patients meeting the 1994 CDC case criteria for CFS. Results of that work are consistent with the view that patients with CFS have a reduction of HPA axis activity due, in part, to impaired central nervous system drive. These observations provide an important clue to the development of more effective treatment to this disabling condition.
————————-
6) edrv.endojournals.org/content/24/2/236.long
Endocrine Reviews April 1, 2003 vol. 24 no. 2 236-252
The Neuroendocrinology of Chronic Fatigue Syndrome
A. J. Cleare, Section of Neurobiology of Mood Disorders, Division of Psychological Medicine, The Institute of Psychiatry, 103 Denmark Hill, London SE5 8AZ,
DHEA and DHEA-S were found to be inversely correlated with depression scores (73 ), and treatment of depressive disorder with DHEA has been successful (74 ). Also of interest is the recent finding that replacement doses of DHEA in Addison’s disease provide benefits to psychological well-being over and above those seen with hydrocortisone replacement
—————————————————–
7) http://www.ncbi.nlm.nih.gov/pubmed/17596739
Neuropsychobiology. 2007;55(2):112-20. Epub 2007 Jun 27.
Hypothalamic-pituitary-adrenal axis function in chronic fatigue syndrome.
Van Den Eede F, Moorkens G, Van Houdenhove B, Cosyns P, Claes SJ. Source Department of Psychiatry, University Hospital Antwerp, Edegem, Belgium.
Abstract There is evidence for a hypofunction of the hypothalamic-pituitary-adrenal (HPA) axis in a proportion of the patients with chronic fatigue syndrome (CFS), despite the negative studies and methodological difficulties. In this review, we focus on challenge studies and on the role of the HPA axis in the pathogenesis of CFS.
Mild hypocortisolism, blunted adrenocorticotropin response to stressors and enhanced negative feedback sensitivity to glucocorticoids are the main findings. Several underlying mechanisms have been proposed. Currently, it is a matter of debate whether these disturbances have a primary role in the pathogenesis of CFS. However, even if the HPA axis dysfunctions are secondary to other factors, they are probably a relevant factor in symptom propagation in CFS.
The fatigue must be accompanied by at least 4 or more of the following case-defining symptoms during at least 6 months of consecutive illness:
sore throat,
tender cervical or axillary lymph nodes,
muscle pain,
multijoint pain,
postexertional malaise,
unrefreshing sleep,
headaches and
impaired memory or concentration
———————————————————————
Clomiphene test for hypothalamic dysfunction
8) endocrinetoday
Comment by Eugene Shippen MD — September 19, 2008 09:12 AM
I totally agree with the author that diagnosis should established before treatment. A short clomiphene stimulation test (clomiphene 25-50mg daily for 7 days followed by FSH/LH testosterone and estradiol) has been forgotten by most clinicians and is absent from most current “Guidelines.”
A robust response which I frequently find insures that the hypogonadism is NOT due to hypothalamic dysfunction that may be due to drugs, disease, lifestyle, alcohol, stress, depression, aging, etc.
Clomiphene testing evaluates both hypothalamic and testicular responses and may lead to most thorough evaluation of the HP axis. The use of low dose clomiphene 10-25 mg 3xweekly in cases with robust response frequently is effective without the need for full testosterone replacement and is sometimes only needed for temporary treatment until the underlying causes are corrected (drugs that suppress testosterone changed, lifestyle improved, alcohol stopped, etc.). Clomiphene has been successfully used in the Lahey Clinic for sexual dysfunction in borderline low testosterone cases (Andre Guay references)
———————————-
9) www.uthsc.edu/endocrinology/documents/ch08-syllabus-Childress.pdf
PATHOPHYSIOLOGY COURSE – ENDOCRINE MODULE
Male Gonadal Disorders (Testicular Disorders & Clinical Conferences)
Dale Childress, MD Monday, December 6, 2010, 8:00-8:50am
Written by: Jeffrey R. Gingrich, M.D.
—————————————————-
10)europepmc.org/abstract/MED/1755138/reload=0;jsessionid=O9H8zAMet60rRRGuY36i.0
Guay AT, Bansal S, Hodge MB Section of Endocrinology, Lahey Clinic Medical Center, Burlington, Massachusetts. Urology [1991, 38(4):317-322]
Effect of raising endogenous testosterone levels in impotent men with secondary hypogonadism: double blind placebo-controlled trial with clomiphene citrate.
Twenty-one men with erectile complaints who were found to have a low level of serum testosterone without a reciprocal elevation of the serum levels of luteinizing hormone were evaluated to identify whether the defect was of hypothalamic or of pituitary origin. Patients underwent a luteinizing hormone (LH)-follicle-stimulating hormone (FSH)-releasing hormone stimulation test that showed a normal but sluggish increase in LH and FSH levels, thus ruling out a pituitary defect and suggesting a suprapituitary abnormality. This was confirmed when, in response to clomiphene, patients had a normal increase in gonadotropin and testosterone levels. Although the basal as well as clomiphene and gonadotropin releasing hormone-stimulated levels of total testosterone and gonadotropins were identical in men less than and more than fifty years old, the elevation of free testosterone levels in response to clomiphene was higher in patients younger than fifty.
This suggested that although the primary abnormality found in these patients is altered secretion of gonadotropin hormone-releasing hormone from the hypothalamus, an age-related decline in the responsivity of Leydig cells to LH may make it more manifest in older patients.
Elevation of testosterone levels from a subnormal to a normal range in response to clomiphene administered for seven days suggests that the defect is functional and reversible and that the drug may be useful in treatment of sexual dysfunction in this group of patients.
———————————
11) www.ncbi.nlm.nih.gov/pubmed/12904801
http://www.nature.com/ijir/journal/v15/n3/full/3900981a.html
Int J Impot Res. 2003 Jun;15(3):156-65. Clomiphene increases free testosterone levels in men with both secondary hypogonadism and erectile dysfunction: who does and does not benefit? Guay AT, Jacobson J, Perez JB, Hodge MB, Velasquez E. Source Center for Sexual Function (Endocrinology), Peabody, Massachusetts 01960, USA.
Abstract Secondary hypogonadism is more common than primary gonadal failure and is seen in chronic and acute illnesses. Although testosterone has a role in erections, its importance in erectile dysfunction (ED) has been controversial. Hypogonadism produced by functional suppression of pituitary gonadotropins has been shown to correct with clomiphene citrate, but with a modest effect on sexual function. We wondered if longer treatment would produce improved results.
A total of 178 men with secondary hypogonadism and ED received clomiphene citrate for 4 months. Sexual function improved in 75%, with no change in 25%, while significant increases in luteinizing hormone (P<0.001) and free testosterone (P<0.001) occurred in all patients. Multivariable analysis showed that responses decreased significantly with aging (P<0.05). Decreased responses also occurred in men with diabetes, hypertension, coronary artery disease, and multiple medication use. Since these conditions are more prevalent with aging, chronic disease may be a more important determinant of sexual dysfunction. Men with anxiety-related disorders responded better to normalization of testosterone. Assessment of androgen status should be accomplished in all men with ED. For those with lower than normal age-matched levels of testosterone treatment directed at normalizing testosterone with clomiphene citrate is a viable alternative to giving androgen supplements.
—–
Clubbing in London
12) blogs.telegraph.co.uk/news/damianthompson/100161244/class-a-clubbing-drugs-your-children-are-taking-them-and-theyre-here-to-stay/
Class A clubbing drugs: your children are taking them and they’re here to stay
By Damian Thompson Health and lifestyle Last updated:
May 29th, 2012
13) www.maps.org/media/esquire_july2012_ecstasy.pdf
MDMA is like a turbo SSRI — it doesn’t just block the transporter, it! reverses the process and floods the!brain with!serotonin. It also works on dopamine levels, which accounts for the energy and stimulation.”
———–
Ecstasy
14) www.ncbi.nlm.nih.gov/pubmed/11888574 www.drugs-forum.com/chemistry/pharmacology/PBB-71-837.pdf
www.erowid.org/archive/rhodium/pharmacology/PBB-71-837.pdf
Pharmacol Biochem Behav. 2002 Apr;71(4):837-44.
Recreational Ecstasy/MDMA, the serotonin syndrome, and serotonergic neurotoxicity. Parrott AC.Department of Psychology, University of East London, E15 4LZ, London, UK. a.c.parrott@uel.ac.uk
Neuroanatomic studies show that the cell bodies are spared, while the long 5-HT axonal projections into the higher brain regions are markedly reduced.
The loss of distal axon terminals in the neocortex and hippocampus is accompanied by a proliferation of axons more proximal to the cell body, or ‘neuronal pruning’ (Fisher et al., 1995).
Neuronal recovery occurs over several months in laboratory rats, whereas monkeys and primates show only partial recovery even after an extended period (Ricaurte et al., 2000).
Verkes et al. (2001) also found a significant reduction in cortisol response to fenfluramine in both moderate and heavy Ecstasy users; their control group being regular ravers/clubbers who had never taken Ecstasy.
——————————————–
15) www.jstage.jst.go.jp/article/jphs/106/1/106_FM0070141/_pdf
www.ncbi.nlm.nih.gov/pubmed/18198474
Pharmacol Sci. 2008 Jan;106(1):2-8. Epub 2008 Jan 16.
Neuropsychotoxicity of abused drugs: molecular and neural mechanisms of neuropsychotoxicity induced by methamphetamine, 3,4-methylenedioxymethamphetamine (ecstasy), and 5-methoxy-N,N-diisopropyltryptamine (foxy). Nakagawa T, Kaneko S. Source Department of Molecular Pharmacology, Graduate School of Pharmaceutical Sciences, Kyoto University, Yoshida, Sakyo-ku, Kyoto, Japan.
Abstract Psychostimulants including amphetamines and cocaine, opioids including morphine, and some recreational drugs share the ability to cause drug dependence and addiction. Although these drugs of abuse primarily act on distinct molecular targets, such as monoamine transporters or receptors, they finally converge to common neural pathways.
Several lines of evidence suggest that their chronic treatment leads to the enhancement of the mesocorticolimbic dopaminergic neurons from the ventral tegmental area (VTA) to the nucleus accumbens (NAc) and the medial prefrontal cortex (mPFC) and leads to abnormal glutamatergic function from the mPFC to the NAc and VTA.
The neural adaptation of dopaminergic-glutamatergic system is considered to be critically implicated in neuropsychotoxic effects of these drugs of abuse.
In addition, recent studies suggest that the serotonergic neurons from the raphe nuclei to limbic areas modulate the mesocorticolimbic dopaminergic-glutamatergic system and participate in the neuropsychotoxicity.
In this review, our recent in vitro studies on the molecular targets and neural adaptation of methamphetamine, 3,4-methylenedioxymethamphetamine (MDMA, “ecstasy”), and 5-methoxy-N,N-diisopropyltryptamine (5-MeO-DiPT, “foxy”) using Xenopus oocytes, organotypic slice cultures of the mesocorticolimbic dopaminergic-glutamatergic system, and the raphe serotonergic system are introduced. Unlike amphetamines or cocaine, MDMA primary acts on SERT as a substrate, rather than DAT and norepinephrine transporter (2).
MDMA causes acute efflux of 5-HT from serotonergic neurons through SERT and leads to a long-term depletion of 5-HT that correlates with destruction of serotonergic nerve Fig. 2.
Preparation of rat organotypic VTA /NAc/mPFC triple slice co-cultures.
A) Illustration of mesocorticolimbic dopaminergic and glutamatergic system. The mesencephalic slice including the VTA, ventral striatal slice including the NAc, and mPFC slice were prepared from postnatal day 3 – 4 rats at a thickness of 350 μm and placed at the air-medium interface on Millicell-CM semiporous membranes. Each of three slices is arranged so that they contacted each other. Slices were maintained in a humidified atmosphere of 5% CO2 and 95% air at 37°C. 6 T Nakagawa and S Kaneko terminals (29, 30)
————————
long term effects of MDMA
16) http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3181923/
Dialogues Clin Neurosci. 2009 September; 11(3): 305–317.
Neurotoxicity of drugs of abuse – the case of methylenedioxy amphetamines (MDMA, ecstasy ), and amphetamines by Euphrosyne Gouzoulis-Mayfrank, Department of Psychiatry and Psychotherapy, University of Cologne, Germany;and Joerg Daumann, Department of Psychiatry and Psychotherapy, University of Cologne, Germany; LVR Clinics of Cologne, Cologne, Germany;
image of ecstasy pills in this article:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3181923/figure/DialoguesClinNeurosci-11-305-g002/
Ecstasy (MDMA) and stimulant amphetamines (METH and AMPPI) are popular drugs of abuse and they are neurotoxic in animal studies. High and repeated doses of MDMA cause selective and long-lasting degeneration of 5-HT axon terminals in several brain regions,
Serotonin-related functions
The neuromodulator 5-1 IT is involved in several functional systems of the CNS. Consequently, damage to the central serotonergic system could be theoretically followed by disturbances in different fields such as psychological well-being, neuroendocrine secretion, vegetative functions, processing of sensory stimuli, sleep architecture, and cognition.
——————————
17) www.ncbi.nlm.nih.gov/pubmed/21444322
J Neurol Neurosurg Psychiatry. 2012 Jan;83(1):83-5. doi: 10.1136/jnnp.2010.228387. Epub 2011 Mar 28.
Preliminary evidence of hippocampal damage in chronic users of ecstasy. den Hollander B, Schouw M, Groot P, Huisman H, Caan M, Barkhof F, Reneman L. Source Graduate School of Neurosciences, Department of Radiology, Academic Medical Center, Amsterdam, The Netherlands.
The hippocampal volume in the ecstasy using group was on average 10.5% smaller than the hippocampal volume in the control group (p=0.032).
These data provide preliminary evidence that ecstasy users may be prone to incurring hippocampal damage, in line with previous reports of acute hippocampal sclerosis and subsequent atrophy in chronic users of this drug.
————-
MDMA and Cortisol- 800% increase in salivary cortisol while clubbing, reduced cortisol long term effects.
18) www.ncbi.nlm.nih.gov/pmc/articles/PMC2826870/
Neuropsychobiology. 2009 November; 60(3-4): 148–158.
Cortisol and 3,4-Methylenedioxymethamphetamine: Neurohormonal Aspects of Bioenergetic Stress in Ecstasy Users A.C. Parrott*
3,4-Methylenedioxymethamphetamine (MDMA) can affect both neurotransmitter and neurohormonal activity.
Cortisol release is increased by stimulatory factors, including physical activity, thermal stress and stimulant drugs. In laboratory studies MDMA leads to an acute cortisol increase of around 150% in sedentary humans. In MDMA-using dance clubbers, the cortisol levels are increased by around 800%, possibly due to the combined factors of stimulant drug, physical exertion and psychosocial stimulation. Regular ecstasy/MDMA users also demonstrate changes in baseline cortisol levels and cortisol reactivity, with compromised hypothalamic-pituitary-adrenal activity. Nonpharmacological research has shown how cortisol is important for psychological aspects such as memory, cognition, sleep, impulsivity, depression and neuronal damage.
Conclusions: The energizing hormone cortisol is involved in the psychobiology of MDMA, probably via its effects on energy metabolism. Acute cortisol release may potentiate the stimulating effects of MDMA in dance clubbers. Chronically, cortisol may contribute to the variance in functional and structural consequences of repeated ecstasy usage. Dance clubbing on ecstasy/MDMA led to an 800% group increase in saliva cortisol, significantly higher than both baseline and dance clubbing during abstinence (fig. (fig.1).1). Gerra et al. [88] noted that the baseline cortisol levels were significantly lower in drug-free ecstasy users compared to controls, along with significantly reduced cortisol responses to a psychosocial stressor. The authors concluded: ‘HPA basal hyperactivation and reduced responsiveness to stress, may represent a complex neuroendocrine dysfunction associated with MDMA use.’
———————-
19) www.alternet.org/story/10482/the_ecstasy_generation
The Ecstasy Generation – Slowly but surely, Ecstasy is becoming the drug of choice for the millennial era. Is it just the ultimate party high, or a postmodern cure that eases spiritual emptiness, rancorous individualism, alienation and lack of community? February 12, 2001
——————-
Image 1 MDMA chemical structure
20) www.ncbi.nlm.nih.gov/pmc/articles/PMC1705495/
Psychopharmacology (Berl). 2007 January; 189(4): 407–424.
Published online 2006 March 16.
3,4-Methylenedioxymethamphetamine (MDMA) neurotoxicity in rats: a reappraisal of past and present findings by Michael H. Baumann, Xiaoying Wang, and Richard B. Rothman Clinical Psychopharmacology Section, Intramural Research Program (IRP), National Institute on Drug Abuse (NIDA), National Institutes of Health (NIH), 5500 Nathan Shock Drive, Baltimore, MD 21224 USA Michael H. Baumann
MDMA targets monoamine transporters, and transporter-mediated release of 5-HT, DA, and NE underlies pharmacological effects of the drug. Consistent with in vitro results, in vivo microdialysis experiments demonstrate that MDMA increases extracellular 5-HT and DA in rat brain, with effects on 5-HT being greater in magnitude Neuroendocrine effects of MDMA include secretion of prolactin from the anterior pituitary and corticosterone from the adrenal glands (Nash et al. 1988).
Evidence indicates that these MDMA-induced hormonal effects are mediated via postsynaptic 5-HT2 receptors in the hypothalamus, which are activated by released 5-HT.
Long Term Adverse Effects of MDMA
The long-term adverse effects of MDMA on 5-HT systems have attracted substantial interest because studies in rats and nonhuman primates show that high-dose MDMA administration produces persistent reductions in markers of 5-HT nerve terminal integrity [reviewed by Lyles and Cadet (2003);
Sprague et al. (1998)]. Table 2 summarizes findings of investigators who first demonstrated that MDMA causes long-term (>1 week) inactivation of tryptophan hydroxylase activity, depletions of brain tissue 5-HT, and reductions in SERT binding and function (Battaglia et al. 1987; Commins et al. 1987; Schmidt 1987; Stone et al. 1987).
These serotonergic deficits are observed in various regions of rat forebrain, including frontal cortex, striatum, hippocampus, and hypothalamus.
Immunohistochemical analysis of 5-HT in cortical and subcortical areas reveals an apparent loss of 5-HT axons and terminals in MDMA-treated rats, especially the fine-diameter projections arising from the dorsal raphe nucleus (O’Hearn et al. 1988).
Moreover, 5-HT axons and terminals remaining after MDMA treatment appear swollen and fragmented, suggesting structural damage.
Long term Damage of MDMA similar to SSRI s
Chronic administration of 5-HT selective reuptake inhibitors (SSRIs), like paroxetine and sertraline, leads to a marked loss of SERT binding and function comparable to MDMA, but these agents are therapeutic drugs rather than neurotoxins (Benmansour et al. 1999; Frazer and Benmansour 2002).
Finally, high-dose administration of SSRIs produces swollen, fragmented, and abnormal 5-HT terminals, which are indistinguishable from the effects of MDMA and other substituted amphetamines (Kalia et al. 2000).
5-HT neurons projecting to the hypothalamus provide stimulatory input for the secretion of adrenocorticotropin (ACTH) and prolactin from the anterior pituitary (Van de Kar 1991).
Accordingly, 5-HT releasers (e.g., fenfluramine) and 5-HT receptor agonists increase plasma levels of these hormones in rats and humans MDMA can produce persistent increases in anxiety-like behaviors without measurable 5-HT deficits suggests that even moderate doses may pose risks.
——————–
21) home.comcast.net/~staticnrg/Cushings/HPA_Drugs.pdf (full pdf file)
http://www.ncbi.nlm.nih.gov/pubmed/18404384
Pituitary. 2008;11(2):219-29.
Drugs and HPA axis. by Ambrogio AG, Pecori Giraldi F, Cavagnini F.
Istituto Auxologico Italiano, Ospedale San Luca, IRCCS, University of Milan, Milan, Italy. This paper outlines the interferences of the most widely used drugs with hypothalamo-pituitary-adrenal function and the related laboratory parameters, with the purpose of providing practical help to clinicians during testing for hypo- or hypercortisolemic states.
22) http://www.modernhcp.com/INNO-PDFS/IMCJ-PDFS/9D9E765C4E354FBAB971EC572EE87198.ashx.pdf
Teitelbaum, Jacob. “Effective treatment of chronic fatigue syndrome.” Integrative Medicine 4.4 (2005): 23-29.
24) http://www.ncbi.nlm.nih.gov/pubmed/18309234
Neuroendocrinology. 2008;88(2):95-102.
The recreational drug ecstasy disrupts the hypothalamic-pituitary-gonadal reproductive axis in adult male rats. Dickerson SM, Walker DM, Reveron ME, Duvauchelle CL, Gore AC.Division of Pharmacology and Toxicology, The University of Texas at Austin
Reproductive function involves an interaction of three regulatory levels: hypothalamus, pituitary, and gonad. The primary drive upon this system comes from hypothalamic gonadotropin-releasing hormone (GnRH) neurosecretory cells, which receive afferent inputs from other neurotransmitter systems in the central nervous system to result in the proper coordination of reproduction and the environment.
Here, we hypothesized that the recreational drug (+/-)-3,4-methylenedioxymethamphetamine (MDMA; ‘ecstasy’), which acts through several of the neurotransmitter systems that affect GnRH neurons, suppresses the hypothalamic-pituitary-gonadal reproductive axis of male rats. Adult male Sprague-Dawley rats self-administered saline or MDMA either once (acute) or for 20 days (chronic) and were euthanized 7 days following the last administration. We quantified hypothalamic GnRH mRNA, serum luteinizing hormone concentrations, and serum testosterone levels as indices of hypothalamic, pituitary, and gonadal functions, respectively.
The results indicate that the hypothalamic and gonadal levels of the hypothalamic-pituitary-gonadal axis are significantly altered by MDMA, with GnRH mRNA and serum testosterone levels suppressed in rats administered MDMA compared to saline. Furthermore, our finding that hypothalamic GnRH mRNA levels are suppressed in the context of low testosterone concentrations suggests that the central GnRH neurosecretory system may be a primary target of inhibitory regulation by MDMA usage.
25) http://www.jneurosci.org/content/19/12/5096.long
http://www.ncbi.nlm.nih.gov/pubmed/10366642?dopt=Abstract
J Neurosci. 1999 Jun 15;19(12):5096-107.
Altered serotonin innervation patterns in the forebrain of monkeys treated with (+/-)3,4-methylenedioxymethamphetamine seven years previously: factors influencing abnormal recovery. by Hatzidimitriou G, McCann UD, Ricaurte GA.
Department of Neurology, The Johns Hopkins Medical Institutions, Baltimore, Maryland 21205, USA.
The recreational drug (+/-)3,4-methylenedioxymethamphetamine (MDMA, “Ecstasy”) is a potent and selective brain serotonin (5-HT) neurotoxin in animals and, possibly, in humans. The purpose of the present study was to determine whether brain 5-HT deficits persist in squirrel monkeys beyond the 18-month period studied previously and to identify factors that influence recovery of injured 5-HT axons. Seven years after treatment, abnormal brain 5-HT innervation patterns were still evident in MDMA-treated monkeys, although 5-HT deficits in some regions were less severe than those observed at 18 months. No loss of 5-HT nerve cell bodies in the rostral raphe nuclei was found, indicating that abnormal innervation patterns in MDMA-treated monkeys are not the result of loss of a particular 5-HT nerve cell group. Factors that influence recovery of 5-HT axons after MDMA injury are
(1) the distance of the affected axon terminal field from the rostral raphe nuclei,
(2) the degree of initial 5-HT axonal injury, and possibly
(3) the proximity of damaged 5-HT axons to myelinated fiber tracts.
Jeffrey Dach MD
7450 Griffin Road, Suite 190
Davie, Fl 33314
954-792-4663
www.jeffreydach.com
www.drdach.com
www.naturalmedicine101.com
www.bioidenticalhormones101.com
www.truemedmd.com
Click Here for: Dr Dach’s Online Store for Pure Encapsulations Supplements
Click Here for: Dr Dach’s Online Store for Nature’s Sunshine Supplements
Web Site and Discussion Board Links:
jdach1.typepad.com/blog/ disc.yourwebapps.com/Indices/244124.html
disc.yourwebapps.com/Indices/244066.html
disc.yourwebapps.com/Indices/244067.html
disc.yourwebapps.com/Indices/244161.html
disc.yourwebapps.com/Indices/244163.html
Disclaimer click here: www.drdach.com/wst_page20.html
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Links to this article: Part One of this series.
Part Two of this series:http://wp.me/P3gFbV-16
Copyright (c) 2013-2014 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page








Clomiphene Clomid Adverse Side Effects Part Three by Jeffrey Dach MD - Jeffrey Dach MD April 26, 2013 at 9:08 AM
[…] Clomid For Men Part Two […]
Hugh Easton June 2, 2013 at 5:05 PM
Sorry to say it, but I think you’re barking up completely the wrong tree here!
I think the main reason why so many people today have problems with endocrine function and sub- or infertility is they were prenatally exposed to high doses of artificial sex hormones, mainly in the course of treatment aimed at preventing miscarriages with either diethylstilbestrol or progestins.
It amazes me how people can get all wound up about things like BPA or pthalates, and yet completely overlook the fact that between 1940 and the mid-1970’s, literally millions of unborn children were inadvertently exposed to often colossally high doses of sex hormone derivatives as a result of these miscarriage treatments.
“The results of the present study clearly document that exposure of the female sheep fetus to androgens during a critical period for sexual differentiation of the brain progressively disrupts reproductive cycles in the adult ewe. Similar effects of androgenization on reproductive function have been described in other species. Specifically, the effects of prenatal androgen exposure have been shown to alter the timing of puberty in female rats (20), guinea pigs (21), and primates (22). In addition, pre- or neonatal testosterone treatment leads to the production of abnormal reproductive cycles in rodents (23) and primates (24), supporting the conjecture that a relatively short exposure to male gonadal hormones early in development can program the reproductive axis of the female to malfunction in later life, leading to sub- or infertility.”
(taken from the discussion section of “Prenatal programming of reproductive neuroendocrine function”, http://www.ncbi.nlm.nih.gov/pubmed/12639926)
Early progestins such as norethisterone were actually derived from the testosterone molecule. Although they’re only weakly androgenic in adults, these testosterone-derived progestins turned out to have strong virilizing effects in the developing fetus (and were eventually withdrawn from use in pregnancy for that reason). If a drug is capable of masculinising the external genitalia of human babies, then it’s highly likely that exposure to it during the critical window of brain development will program the reproductive axis to malfunction later in life and create the human equivalent of the sheep in that experiment.
Progestins were and are widely used in pregnancy, so there must be a lot of women around with reproductive problems due to prenatal progestin exposure. Is it the cause of polycystic ovary syndrome I wonder?
Theoretically there should be a reverse effect too: in a pregnancy where the unborn infant is male, and exposure to drugs that interfere with testosterone production takes place (that’s what I think happened in my case). I’ve recently obtained copies of the family photos from my childhood, and in them it’s clear that by my early teens I was already developing the “eunuchoid” body structure and feminine appearance I have today – long before any recreational drug use took place. Based on what I’ve seen among DES sons, it certainly seems that prenatal exposure to artificial sex hormones can give rise to hypogonadism, endocrine problems and sub- or infertility in men as well as women later in life.
All in all there seems to be a colossal unrecognised problem with the use of these substances in pregnancy!
google June 14, 2013 at 3:29 PM
google…
G http://images.google.com.hk/…
B12 Deficiency and Neuro-Psychiatric Disorders by Jeffrey Dach MD - Jeffrey Dach MD April 25, 2014 at 7:58 AM
[…] Clomid For Men With Low Testosterone, Part Two […]
Clomid for men with low testosterone part four November 28, 2014 at 3:40 PM
[…] Clomid For Men With Low Testosterone, Part Two […]