





 PCOS Polycystic Ovary Syndrome
PCOS Polycystic Ovary Syndrome
Anovulatory Androgen Excess, Part One
by Jeffrey Dach MD
This article is Part One of a series,
For Part Two, Click Here.
Alice is a 17 tyar old high school student and has Polycystic Ovary Syndrome, PCOS. She has about one menstrual cycle per year since age 13, and has never really started normal cycles.
Alice is overweight, and has facial hair and acne caused by elevated testosterone levels. Alice’s OB/Gyne doctor diagnosed PCOS (Polycystic Ovary Syndrome), and prescribed birth control pills to regulate her cycles. The birth control pills caused adverse side effects of weight gain weight and elevated blood pressure (hypertension), so Alice stopped them.
Upper image courtesy of wikimedia commons.
Progesterone – the Most Logical Form of Treatment
Actually Works
Two months ago, Alice was switched over from the birth control pills to natural progesterone, taking a 100 mg capsule twice a day for 14 days on, 14 days off. The progesterone was successful, restoring a normal menstrual period, and a return to regular cycles.
BCP’s (birth control pills) are commonly prescribed by the mainstream OB/Gyne doctor or pediatric endocrinologist to regulate cycles in the PCOS patient. This treatment is not the best one. There is a better more logical tresatment called natural progesterone. Both John R Lee MD, and JeriLynn Prior MD advocate the use of natural progesterone as a far better alternative to birth control pills. After all, birth control pills (BCP’s) are a chemical form of castration, and work by inhibiting ovulation.
This article will explain the cause of PCOS, and will describe the signs and symptoms of PCOS, including the clinical features of PCOS, and give you a simple questionnaire to determine if you have PCOS. This article will also explain why natural progesterone is the best treatment, and a much better choice compared to birth control pills.
PCOS was Rare When First Described in 1935, Now Quite Common.
When PCOS (polycystic ovary syndrome) was first described in 1935 by Stein and Leventhal, it was fairly rare.(55) Nowadays, it is quite common, involving 6 to 10 per cent of the female population, affecting 3.5 to 5 million women. (24) Why the increased incidence? Some believe that endocrine disruptor chemicals in the environment are to blame.(60A)

Clinical Signs and Symptoms Of PCOS
1) Oligomenorrhea or amenorrhea (no periods), Anovulation (no ovulation)
2) Weight gain, obesity, Hirsutism (excessive hair growth, male pattern)
3) Insulin resistance (pre-diabetes),
4) Acne,
5) Male-pattern baldness,
6) Multiple small ovarian cysts on sonogram,
7) Acanthosis Nigrans (darkening of the skin at the nape of the neck and under arms)-indicator of hyperinsulinemia
Above Left Image: Obese Young Lady with PCOS, anovulatory infertility, acne and facial hair.
A Brief Moment for Definitions:

Hirsutism
Definition of ovulation: This is the when an egg pops out of the follicle in the ovary, and starts on the long trip down the fallopian tube to the uterine cavity where it can be fertilized to form a new baby. Ovulation causes high progesterone production by corpus luteum in the ovary. Menstrual Cycles are regular.
Definition of Anovulation: The egg doesn’t’t pop out and there is no progesterone production. The cycles are irregular or absent.
Above Left Image: Typical hirsutism, with hair growth under the chin.

Hirsutism
How Do You Know If You Have PCOS?
This is the PCOS Questionnaire.(63)(64) and these are the Links to questionnaire articles:
2) PCOS questionnaire
If you answer Yes, to 2 out of 3 of the following questions, this indicates high likelihood (80%) of PCOS.
Above Left Image: The bearded fat lady at the circus. She had PCOS.
Length of Menstrual Cycle, Variable Length
1) Between the ages of 16 and 40, was length of your menstrual cycle (on average) greater than 35 days and/or totally variable ?
Hair Growth (Male Pattern)
2) During your menstruating years (not including during pregnancy), did you have dark, coarse hair on your three or more of these sites? Upper lip? chin? breasts? chest between the breasts? back? belly? upper arms? upper thighs?
Obesity
3) Were you ever obese or overweight between the ages of 16 and 40?

Hormone Levels during the Menstrual Cycle with normal ovulation.
The green dotted line is progesterone which rises days 14-22.
The progesterone is absent in PCOS, because there is no ovulation,
and the green line stays flat on the chart, instead of rising
The world’s greatest authority, Leon Speroff MD, says: “A question which has puzzled gynecologists and endocrinologists for many years is what causes polycystic ovaries. There is an answer which is appealing in its logic and clinical applicability. The characteristic polycystic ovary emerges when a state of anovulation persists for any length of time”
(1) Clinical Gynecologic Endocrinology and Infertility by Leon Speroff MD p.493
PCOS is the end result of not ovulating, (no progesterone production) for a long time (a few years), resulting in a vicious cycle which self perpetuates anovulation, causing increased testosterone production by the ovary. Insulin resistant diabetes and obesity aggravate the problem. As you might expect, PCOS is a major cause of infertility.
About 10% of patients thought to have PCOS actually have an underlying genetic enzyme defect in adrenal steroid synthesis called Non-Classical CAH. This can be diagnosed with a Cortrosyn stimulation test, and a 21-OH genetic test called CAHDtex from Esoterix. If present, treatment is successful with low dose adrenal steroid tablets (cortef, dexamethasone, prednisone) which restores fertility and reverses the acne. (see below discussion on non-classical CAH).
Oral Contraceptives for PCOS (BCP’s)
Birth control pills are a chemical form of castration, which prevent ovulation. Lack of ovulation is the primary defect in PCOS, so birth control pills merely perpetuate the primary defect. Birth control pills can restore regular bleeding periods, however, this is artificial, and aggravate the underlying PCOS problem rather than solve it. In addition, birth control pills are known to worsen insulin resistance and diabetes. (2)
“PCOS may affect between 3.5 and 5.0 million young women in the United States, it arguably may be the most important general health issue affecting young women. BCP’s (OCPs) are the traditional therapy for the chronic treatment of PCOS…… limited evidence raises the issue that BCP’s (OCPs) may aggravate insulin resistance and exert other untoward metabolic actions that possibly enhance the long-term risk for diabetes and heart disease.”

JL Prior
JeriLynn Prior MD Says:“The fundamental problem with PCOS is not making progesterone for two weeks every cycle. This lack of progesterone leads to an imbalance in the ovary, causes the stimulation of higher male hormones and leads to the irregular periods and trouble getting pregnant. Progesterone is usually missing—replacing it therefore makes sense. “

Self-Medication Not Recommended
Some young women find out about progesterone on internet messenger boards, and then proceed on their own to buy it over-the-counter. The progesterone cream may successfully restores cycles in many cases. However, self – medication is not recommended. It is best to work with a knowledgeable physician. If you have PCOS and need a doctor to prescribe progesterone, you can find a knowledgeable physician on the ACAM or A4M doctor’s directory.(65)(66) Always work closely with a knowledgeable physician.
Can PCOS be Treated with Natural Progesterone?
YES by Dr. Jerilynn Prior (3)
“Progesterone talks back to the hypothalamic and pituitary (brain) hormones that control the ovaries and stops them from stimulating the ovaries to make too much testosterone.”
Dr Prior recognizes that the (BCP) pill, with its synthetic type of progesterone, does help women with PCOS to a certain degree.
But her goal for PCOS patients is, “to return the brain/ovary system to a normal balance. The goal of the BCP Pill is the opposite – it must suppress the brain-ovary system to prevent pregnancy.”
To help her PCOS patients achieve a normal hormonal balance, she prescribes oral micronized progesterone (trade name Prometrium) which is a bio-identical hormone. Taking this natural progesterone for two weeks every month (called cyclic progesterone therapy) may help the brain to develop the normal cyclic rhythm that is missing in PCOS.
Interestingly, Dr. Prior believes there is another benefit of cyclic progesterone therapy. She explains, “most doctors don’t realize progesterone antagonizes and inhibits the enzyme (called 5-alpha reductase) that is needed to make testosterone into dihydrotestosterone. Dihydrotestosterone is the powerful male hormone that talks hair follicles into making coarse hair and too much oil that causes acne.”
Above quote is attributed to Jerilyn Prior MD Web Site.(3)
___________________________________________________________

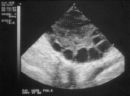
PCOS Ultrasound showing ovarian cysts

WHAT MAKES YOUR OVARIES TICK Insights about Ovulation, Fertility, PCOS and more. (4)
Click Here for an Interview with Jerilynn C. Prior, M.D. posted on the Virgina Hopkins Health Watch. Dr. Jerilynn Prior is a professor of endocrinology at the University of British Columbia. She is a pioneer in research involving women’s menstrual cycles, ovulation, progesterone and bone loss.
Above Left Image: Polycystic ovary on ultrasound image.
Interview Quoted from Virgina Hopkins Health Watch:
JLML: How do you track your luteal phase with a basal temperature chart?
JCPrior: If you record your oral temperature every morning for an entire month using a digital thermometer, record the temperature in the evening before you go to bed, and record any illness or early or late rising, you can quantitatively determine which days of the cycle are high progesterone days. You can then take all of those daily temperatures from the beginning of one period until the day before the beginning of the next, and do an average of the temperatures. The point where your temperature goes above that average, and stays above it, is the beginning of the luteal phase. It will go back down when your period starts or just before. That’s how easy it is to figure out your luteal phase length! That alone is valuable information for women who are having miscarriages that may be due to a short luteal phase.
JLML: I have found that women who are more aware of their cycles are often better able to self-treat for hormone imbalances.
JLML: What else can you tell us about anovulatory cycles? The other kind of ovulation disturbance I called “turned on.” The woman experiencing this kind of ovulation disturbance will complain of weight gain, acne, and hair where she doesn’t want it. The biology of this is less clear, but it relates to insulin excess and insulin resistance, which have effects both on the brain by increasing LH (luteinizing hormone) levels, and directly on the ovary. Excess insulin sits on receptors on the theca cells, the outer coat of the ovary, and makes them more responsive to the hormonal environment, and therefore they make more androgens [testosterone, male hormones].
JLML: Aha! So that’s why a high sugar diet aggravates polycystic ovary syndrome. The excess sugar creates high insulin levels, which stimulate androgen production in the ovary, which suppresses ovulation.
JCPrior: The higher LH and the higher androgen levels set up a signal that inhibits the follicle from ovulating. Because each follicle grows and creates a lake of fluid around it, if it doesn’t burst and release its egg, a cyst is left. Therefore you get into a situation of high or normal estrogen levels, high androgens, and low progesterone. That condition is usually characterized by obesity, especially middle-of-the-body obesity, androgen signs such acne, oily skin, facial and breast hair, and head hair loss. Because estrogen tends to be higher with weight gain, these are the women who have a higher breast cancer and endometrial cancer risk. They may also have the worst PMS symptoms.
JLML: So this is yet another good reason to avoid sugar and refined carbohydrates such as white bread and pasta.
JCPrior: And it’s another good reason to get plenty of aerobic or endurance-type exercise, which is one of the best ways of getting the insulin levels down and decreasing PMS. With turned on ovulation disturbances you need to correct three problems: The first is to bring progesterone into balance –and for this you use physiologic doses of progesterone. Next, you often you need to block the effect of the male hormone. There’s a medicine called spironolactone which I use that blocks androgen action at the cell level. Finally, if a person has a family history of diabetes or is quite obese, then I may use a drug called metformin (Glucophage) that sensitizes the body to insulin and allows the insulin levels to go down.
JLML: I have found that supplemental progesterone, a good amount of exercise, and a low sugar diet, low simple carbohydrate and low fat diet with plenty of vegetables will often restore balance.
The above interview posted courtesy of Virginia Hopkins Health Watch. (4)
Help for PCOS – Cyclic Progesterone Therapy by Dr. Jerilynn C. Prior and Celeste Wincapaw (5)
Jerilynn C. Prior MD Says:
I use cyclic progesterone therapy as the heart of treatment for PCOS- anovulatory androgen excess.(6) Progesterone is the hormone made by the ovary after an egg is released.
The fundamental problem with PCOS is not making progesterone for two weeks every cycle. This lack of progesterone leads to an imbalance in the ovary, causes the stimulation of higher male hormones and leads to the irregular periods and trouble getting pregnant. Progesterone is usually missing—replacing it therefore makes sense. Progesterone talks back to the hypothalamic and pituitary (brain) hormones that control the ovary, and stops them from stimulating the ovary to make too much testosterone.
Taking progesterone for two weeks every month (called cyclic progesterone) may help the brain to develop the normal cyclic rhythm that is missing in PCOS. Progesterone also counterbalances the steadily high estrogen levels that the PCOS ovary produces even if you have no periods. Progesterone will prevent estrogen over-stimulation of the uterine lining (endometrial hyperplasia) and heavy flow. It may also interfere with the action of high estrogen on the breasts, therefore preventing tenderness and “lumpiness” and perhaps even the risk for breast cancer.
Finally, and most doctors don’t realize this, progesterone antagonizes and inhibits the enzyme (called 5-alpha reductase) that is needed to make testosterone into dihydrotestosterone. Dihydrotestosterone is the powerful male hormone that talks hair follicles into making coarse hair and too much oil that causes acne.
Useful Tools for Patients:
Protocol for Cyclic PROGESTERONE THERAPY patient handout sheet (6)
Menstrual cycle diary log sheet patient handout (7)
________________________________________________________________
Guidelines for Progesterone Cream Dosage for PCOS (8)
Early PCOS – 32mg from day 12-26
Advanced PCOS – 54mg from day 12-26 of your cycle
Severe PCOS with pain, 64mg of progesterone cream from day 5-26 , to address pain from endometriosis. Then try to wean back to a lesser dose or to extend breaks to fall into line with a day 12-26 cycle. Note, if you are using a regime day 5-26 in the first 4-7 months until symptoms settle, please be aware you are using a program suggested to enhance fertility. (8)
_______________________________________________________
Dr. Lam Progesterone Guidelines for Polycystic Ovary Syndrome (9)
Dr. Lam follows Dr John R Lee pioneering use of progesterone.
Apply 20 mg of progesterone cream during day 14 to 28 of the menstrual cycle. Adjust accordingly if for longer or shorter cycle. As the hormonal balance is regained, facial hair and acne, two commonly associated symptoms, will disappear. (9)
_________________________________________________________
Other treatable causes of anovulation
1) Low thyroid function (hypothyroid) causes menstrual irregularity, anovulation and infertility. Ovulation and fertility is restored by thyroid medication. Ovarian cysts also resolve.
2) Vitamin D deficiency is associated with anovulation. Resolves with Vitamin D.
3) Iodine deficiency causes ovarian cysts and anovulation, reversed by iodine supplementation.
_________________________________________________
Other Useful Drug Treatments for PCOS:
Issue Drug Treatment
Infertility, anovulation: Clomid clomephine, induces ovulation.
Insulin Resistance: Metformin improves insulin sensitivity.(39)(39A)
Acne, Facial Hair: Spironlactone, Aldactone inhibits testosterone.
__________________________________________________________
PCOS—polycystic ovary syndrome.
Standard diagnostic assessments:
1) History may show: Variable or anovulatory menstrual pattern, obesity, hirsutism, and the absence of breast discharge.
2) Pelvic sonogram may show: 10 or more cysts in each ovary, ‘string of pearls’.
The ovaries are generally 1.5 to 3 times larger than normal.
3) Labs may show:
Elevated DHEAs and free testosterone.
Ratio of LH to FSH is greater than 1:1, as tested on Day 3 of the menstrual cycle.
The pattern is not very specific and was present in less than 50% in one study.
Common assessments for associated conditions or risks.
1) Fasting biochemical screen and lipid profile
2) 2-hour oral glucose tolerance test (GTT) in patients with risk factors (obesity, family history, history of gestational diabetes) and may indicate impaired glucose tolerance (insulin resistance) in 15-30% of women with PCOS. Frank diabetes can be seen in 65–68% of women with this condition. Insulin resistance can be observed in both normal weight and overweight patients.
Lab tests for exclusion of other disorders that may cause similar symptoms:
1) Prolactin
2) TSH
3) 17-hydroxyprogesterone to rule out 21-hydroxylase deficiency (CAH).
4) Fasting insulin level or GTT with insulin levels (also called IGTT).
5) Fasting Glucose to Fasting Insulin ratio <4.5 is cheaper method
ICD-9 Codes: PCOS ICD-9 256.4 Amenorrhea ICD-9 626.0
__________________________________________________________________
This article is Part One of a series,
For Part Two, Click Here.
Non Classical CAH Congenital Adrenal Hyperplasia,
also known as Non-Classical 21 Hydroxylase Deficiency (NC21OHD)
Non-Classical CAH or 21 Hydroxylase Deficiency is the most common genetic disease known, occurring in 1% of New Yorkers, and up to 3% in ethnic groups such as of Ashkenazi Jews, Hispanics, Italians, and Yugoslavs.(68)
Ten per cent of patients with PCOS actually have Non-Classical CAH. The underlying genetic defect causes an enzyme deficiency in the adrenal gland which reduces the ability of the adrenal to make cortisol. Instead of making cortisol, the adrenal steroid pathways are shunted towards testosterone causing elevated testosterone and the typical symptoms of hair growth (hirsutism), and acne and there may also be menstrual irregularities, anovulation, and infertility.(69)(70)
What is the 21 Hydroxylase Enzyme?
This is a key enzyme in the adrenal gland which converts cholesterol into cortisol. In the Classical form of CAH, the 21 hydroxylase enzyme (21-OH) is severely deficient with resulting low cortisol levels. In the Non-Classical form however, the 21 hydroxylase (21-OH) enzyme is still working fairy well with only a slight reduction in activity, and cortisol levels are usually normal, while testosterone levels may be elevated to a variable degree. The Human Adrenal Steroid synthesis pathways and the adrenal enzymes involved can be understood on this chart from Quest Labs.(71)
How to Make the Diagnosis of Non-Classical CAH? Cortrosyn Stimulation
The most definitive diagnosis is done with a Cortrosyn Stimulation test (0.25 mg) which measures 17-hydroxyprogesterone (17-OHP) at 0 and 60 minutes after SQ injection of the Cortrosyn (ACTH).
This test in simple terms is described here:
First a preliminary (baseline ) blood test is done for various hormones including 17-OH, this is followed by a subcutaneous injection of 0.25 mg of a drug called Cortrosyn which is a form of ACTH which stimulates the adrenal glands to make more hormones. An hour (60 minutes) after the Cortrosyn injection, a post stimulation blood sample is drawn for lab testing for 17-OH and other hormones.
Patients with Non Classic 21-OH Deficiency typically show 60-min stimulated 17-OHP values between 1,500 and 10,000 ng/dl. This chart shows how the 17-OHP values cluster at three areas for normal (below 1,500), Non-Classical CAH (1500-10,000) and, and Classical CAH (above 10,000). (72) The Quest Lab testing algorithm is shown here.(73)
Genetic Testing for 21-OH Deficiency
Genetic testing is now available and very useful. This test shows whether or not there is a mutation in the CYP21A2 gene coding for the 21-Hydroxylase Enzyme.(74) The CAHDtex test by Esoterix is useful in showing the exact mutation in the CYP21A2 gene. (75) Once the exact mutation in the CYP21A2 gene is known, refer to this chart to determine the severity of the enzyme defect.(76) Genetic testing of other family members is usually recommended once a sibling is found with the mutation.
Clinical Presentation in Children
In children, the signs include premature onset of puberty, cystic acne, accelerated growth, and advanced bone age. Premature development of pubic hair may occur as early as 6 months of age (due to elevated testosterone). The severe cystic acne may be unresponsive to oral antibiotics and retinoic acid (Accutane).
Although the child may be taller than the other kids in early childhood, this early growth spurt finishes early (because of epiphyseal fusion), and final height ends up shorter than usual. Thus, these kids are tall children but short adults.
Another feature may be male pattern baldness in a female involving the top of the head and sparing the sides.
Teenagers and Young Adults – Major Cause of Infertility
Teenage girls may present with features of elevated testosterone such as facial hair (hirsutism), acne and menstrual irregularities or anovulation. Young adult females may present with the chief complaint of infertility. It has been generally recognized that infertility of undetermined cause in women may be reversed with glucocorticoid (cortef or prednisone) therapy, which most likely treats an occult Non-Classical CAH Syndrome. William Mc Jefferies MD successfully treated thousands of such cases ( The Safe Uses of Cortisol).(77)
Treatment of Non Classical CAH with Cortisol Restores Fertility
Oral tablets containing low dose cortisol sucessfully treat Non-Classical CAH and reverse the symptoms restoring fertility. The cortisol suppresses ACTH and reduces the testosterone production by the adrenal.
Dr. Maria New has followed a large group of 400 patients with Non-Classical CAH, and she treats them with 0.25 mg dexamethasone at the hour of sleep, and she notes it takes about 3 months for reversal of acne and infertility. Hirsutism takes longer to respond, about 30 months.
The cost for a dexamethasone tablet is $0.50, and the 3-month treatment cost is estimated to be $45. Compare this $45 dollars to the infertility treatment cost of $30,000 for one cycle of in vitro fertilization . Dr. Maria New says that many patients presenting with infertility actually have NonClassical CAH, and fertility could be restored easily with treatment with oral cortisol tablets such as cortef, dexamethasone, or prednisone. (69) Before you spend a fortune on in-vitro fertilization for infertility, it would be prudent to rule out Non-Classical CAH with a simple genetic test. For more information on CAH, see my article on this topic: A Commonly Missed Cause of Infertility, NonClassical CAH by Jeffrey Dach MD (78)
This article is Part One of a series,
For Part Two, Click Here.
Jeffrey Dach MD
www.drdach.com
www.jeffreydach.com
www.drdach.com
www.naturalmedicine101.com
www.truemedmd.com
Link to this article: http://wp.me/P3gFbV-7p
http://jeffreydach.com/2008/02/13/understanding-pcos-the-hidden-epidemic-by-jeffrey-dach-md.aspx
REFERENCES
(1) http://www.amazon.com/Clinical-Gynecologic-Endocrinology-Infertility-Editorial/dp/0781747953
The Clinical Gynecologic Endocrinology and Infertility: Leon Speroff MD
(2) http://jcem.endojournals.org/cgi/content/full/88/5/1927
A Modern Medical Quandary: Polycystic Ovary Syndrome, Insulin Resistance, and Oral Contraceptive Pills, The Journal of Clinical Endocrinology & Metabolism Vol. 88, No. 5 1927-1932
(3) http://www.pcosupport.org/newsletter/articles/article122707-3.php
Can PCOS be Treated with Natural Progesterone? Jerilynn Prior, PCOSA Today Newsletter
(4) http://www.virginiahopkinstestkits.com/priorovaries.html
WHAT MAKES YOUR OVARIES TICK, Insights about ovulation, fertility, PCOS and more.An Interview with Jerilynn C. Prior, M.D. FRCPC
(5) http://www.cemcor.ubc.ca/help_yourself/articles/challenge_pcos
Help for Anovulatory Androgen Excess (AAE)—Challenge PCOS! by Dr. Jerilynn C. Prior and Celeste Wincapaw
(6) http://www.cemcor.ubc.ca/files/uploads/Cyclic_Progesterone_Therapy.pdf
INFORMATION FOR WOMEN: CYCLIC PROGESTERONE THERAPY Protocol for treatment.
(7) http://www.cemcor.ubc.ca/files/uploads/Menstrual_Cycle_Diary_with_treatments.pdf
Menstrual Cycle Diary / Log Book / Calendar
(8) http://www.natural-progesterone-advisory-network.com/
what-is-the-guidelines-to-progesterone-dosage/
What is the guidelines to progesterone dosage for PCOS ? National Progesterone Advisory Network
(9) http://www.drlam.com/A3R_brief_in_doc_format/progesterone.cfm
Dr. Lam Progesterone Page
(10) http://www.virginiahopkinstestkits.com/pcos.html
What Your Dr. May Not Tell You about PCOS, Polycystic Ovary Syndrome (PCOS), A New Epidemic that Causes Infertility, Excess Hair, Acne and More By John R. Lee, M.D. and Virginia Hopkins
(11) http://www.townsendletter.com/Nov2004/phyto1104.htm
Townsend Letter, Phytotherapy for Polycystic Ovarian Syndrome (PCOS) by Angela Hywood N.D. & Kerry Bone, Townsend Letter message Boards
(12) http://pcos.meetup.com/217/
PCOS GROUPS and Message Boards, The Arizona Polycystic Ovarian Syndrome Meetup Group,
(13) http://search.yahoo.com/
search?p=pcos+message+board&fr=yfp-t-501-s&toggle=1&cop=mss&ei=UTF-8
Hundreds of PCOS Message Boards
(14) http://www.early-pregnancy-tests.com/vitex.html
Home Ovulation Tests, Pregnancy Test Kits, Basal Thermometers
Birth Control Pills
(15) http://www.sensible-alternative.com.au/polycystic_ovarian_syndrome.html
The Birth Control Pill is NOT the Answer. The birth control pill does absolutely nothing to improve insulin resistance, and can actually worsen it
(1). “They may, however, worsen insulin resistance and lead to deterioration of glucose tolerance.” Glucose tolerance deteriorated significantly, and two women developed diabetes” In 2003, the Journal of Clinical Endocrinology & Metabolism published an article called ‘A Modern Medical Quandary: Polycystic Ovary Syndrome, Insulin Resistance, and Oral Contraceptive Pills’.
(2) The Pill has been standard treatment for PCOS, and yet, perversely, it appears to worsen the metabolic problem that is at the root of the condition. The authors say:
‘…what has been lacking is a critical examination of whether oral contraceptives might…exert adverse metabolic effects with long-term consequences..’.
I propose that the Pill has made additional contributions to the epidemic of PCOS. The Pill is known to cause permanent hormone changes, even once it is stopped.
(3). Most doctors agree that it can take 1 to 2 years for normal menstrual cycles to resume after stopping the pill . The pill will cause a monthly bleed, but this is not a true period.
(16) http://jcem.endojournals.org/cgi/content/full/82/9/3074
The Journal of Clinical Endocrinology & Metabolism Vol. 82, No. 9 3074-3077. The Effect of a Desogestrel-Containing Oral Contraceptive on Glucose Tolerance and Leptin Concentrations in Hyperandrogenic Women Shahla Nader, Maggy G. Riad-Gabriel and Mohammed F. Saad
(17) http://jcem.endojournals.org/cgi/content/full/88/5/1927
Diamanti-Kandarakis, E et al. A modern medical quandary: Polycystic Ovary Syndrome, Insulin Resistance, and Oral Contraceptive Pills. J Clin End Met 2003.88(5): 1927-1932 CONTROVERSIES IN ENDOCRINOLOGY Evanthia Diamanti-Kandarakis, Jean-Patrice Baillargeon, Maria J. Iuorno, Daniela J. Jakubowicz and John E. Nestler
(18) http://www.ncbi.nlm.nih.gov/pubmed/16409223
Panzer et al. Impact of Oral Contraceptives on Sex Hormone-Binding Globulin and Androgen Levels: A Retrospective Study in Women with Sexual Dysfunction. The Journal of Sexual Medicine. 2006. 3:p.104-113
(19) http://www.eurekalert.org/pub_releases/2006-01/bpl-ocp121305.php
Birth Control Pill Side effects. Oral contraceptive pill may prevent more than pregnancy
New research indicates birth control pill could cause long-term problems with testosterone
(20) http://ditchthepill.org/
Ditch the Pill . org, very neative about BCPs
Jones, M.D. Medical Director, Women’s Health Institute
THYROID References
(21) http://www.ncbi.nlm.nih.gov/pubmed/16208308?dopt
Abstract Minerva Endocrinol. 2005 Sep;30(3):193-7. Relationship between insulin secretion, and thyroid and ovary function in patients suffering from polycystic ovary. CONCLUSIONS: The data obtained in our study enable us to support the close connection between ovary function, thyroid function and insulin-resistance. In all patients, in fact, albeit at different times, an improvement was obtained in all 3 pathologies.
(22) http://www.ncbi.nlm.nih.gov/pubmed/17302862
Thyroid disease and female reproduction. Poppe K, Velkeniers B, Glinoer D. Clin Endocrinol (Oxf). 2007 Mar;66(3):309-21
(23) http://www.ncbi.nlm.nih.gov/pubmed/15012623
High prevalence of autoimmune thyroiditis in patients with polycystic ovary syndrome.Janssen OE. Eur J Endocrinol. 2004 Mar;150(3):363-9. CONCLUSION: This prospective study demonstrates a threefold higher prevalence of Autoimmune Thyroid disorders in patients with PCOS
Prevalence of PCOS in Population
(24) http://jcem.endojournals.org/cgi/content/full/85/7/2434
A Prospective Study of the Prevalence of the Polycystic Ovary Syndrome in Unselected Caucasian Women from Spain. Our results demonstrate a 6.5% prevalence of PCOS, as defined, in a minimally biased population of Caucasian women from Spain. The polycystic ovary syndrome, hirsutism, and acne are common endocrine disorders in women. The Journal of Clinical Endocrinology & Metabolism Vol. 85, No. 7 2434-2438
Thyroid References
(25) http://www.ncbi.nlm.nih.gov/pubmed/8053991
Hypothyroidism presenting with polycystic ovary syndrome.Sridhar GR. J Assoc Physicians India. 1993 Feb;41(2):88-90. During a 30 months period, two women of primary hypothyroidism (2/13; 1.04%) presented with features of polycystic ovary syndrome (PCOS). In hypothyroidism, sex hormone binding globulin levels are decreased; increased conversion of androstenedione to testosterone, and aromatization to estradiol are present, all these being an exaggeration of biochemical changes characteristic of PCOS. Besides, metabolic clearance rates of androstenedione and estrone, the putative mediators of PCOS, are reduced. Hypothyroidism can either initiate, maintain or worsen the syndrome. Correction of hypothyroidism when present, would therefore form an important aspect in the management of infertility associated with PCOS.
(26) http://www.ncbi.nlm.nih.gov/pubmed/17954423
Precocious puberty and large multicystic ovaries in young girls with primary hypothyroidism.Sanjeevaiah AR, Sanjay S, Deepak T, Sharada A, Srikanta SS. Samatvam Endocrinology Diabetes Center, Bangalore, India.
(27) http://www.ncbi.nlm.nih.gov/pubmed/17917634
Mymensingh Med J. 2007 Jul;16(2 Suppl):S60-62. Vaginal bleeding with multicystic ovaries and a pituitary mass in a child with severe hypothyroidism.Mohsin F, Nahar N, Azad K, Nahar J. Department of Paediatrics, Bangladesh Institute of Research and Rehabilitation on Diabetes, Endocrine and Metabolic Disorders (BIRDEM), Dhaka, Bangladesh.
A seven year and ten months old girl presented with cyclic vaginal bleeding and a huge abdominopelvic mass. She had clinical features of hypothyroidism. The investigation results were consistent with the diagnosis of primary hypothyroidism with precocious puberty. She also had bilaterally enlarged cystic ovaries on CT scan of abdomen and CT scan of brain showed pituitary macroadenoma. After starting treatment with thyroxine, patient became euthyroid and her general condition improved. Treatment with thyroxine alone halted the cyclic vaginal bleeding, led to rapid resolution of the ovarian cysts and regression of the pituitary mass.
(28) http://www.ncbi.nlm.nih.gov/pubmed/2729396
Spontaneous ovarian hyperstimulation syndrome associated with hypothyroidism. Rotmensch S, Scommegna A. Department of Obstetrics and Gynecology, Michael Reese Hospital and Medical Center, University of Chicago, Pritzker School of Medicine, IL 60616. Am J Obstet Gynecol. 1989 May;160(5 Pt 1):1220-2.
(29) http://www.ncbi.nlm.nih.gov/pubmed/17954423?ordinalpos=4&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_RVDocSum
Precocious puberty and large multicystic ovaries in young girls with primary hypothyroidism.Sanjeevaiah AR, Sanjay S, Deepak T, Sharada A, Srikanta SS. Endocr Pract. 2007 Oct;13(6):652-5.
(30) http://www.ncbi.nlm.nih.gov/pubmed/16864150
Primary hypothyroidism presenting as ovarian tumor and precocious puberty in a prepubertal girl.Campaner AB, Scapinelli A, Machado RO, Dos Santos RE, Beznos GW, Aoki T. Department of Obstetrics and Gynecology, Santa Casa São Paulo-Faculty of Medical Science, São Paulo, Brazil. Gynecol Endocrinol. 2006 Jul;22(7):395-8.
We report a case of a prepubertal girl with juvenile primary hypothyroidism presenting as ovarian cysts and precocious puberty. The 7-year-old female was referred to our clinic because of a pelvic/abdominal mass and vaginal bleeding. Besides these findings, on physical examination we noticed the thyroid gland globally increased and the presence of secondary sexual characteristics. Based upon the clinical profile and investigations, the patient was diagnosed with juvenile primary hypothyroidism due to autoimmune thyroiditis. The cysts and precocious puberty resolved spontaneously after the simple replacement of thyroid hormone. It is important to bear in mind hypothyroidism in cases of girls presenting ovarian cysts and precocious puberty in order to avoid unnecessary surgery on the ovaries.
(31) http://www.ncbi.nlm.nih.gov/pubmed/16995569
J Pediatr Endocrinol Metab. 2006 Jul;19(7):895-900.
Ovarian cysts in young girls with hypothyroidism: follow-up and effect of treatment.Sharma Y, Bajpai A, Mittal S, Ovarian cysts have been reported in girls with longstanding uncompensated primary hypothyroidism. Restoration of euthyroid state has been associated with resolution of these cysts; long-term follow-up of these patients is however lacking. Our study emphasizes the need to exclude hypothyroidism in young girls with ovarian cysts. A causal link between hypothyroidism and spontaneously occurring ovarian hyperstimulation syndrome is suggested by analysis of data from a patient with myxedema and review of data from animal research.
(32) http://www.jacemedical.com/articles/Sub-laboratory%20Hypothyroidism%20.pdf
“Sub-laboratory” Hypothyroidism and the Empirical use of Armour® Thyroid Alan R. Gaby, MD . Excellent revierw on subclinical hypothyroidism.
“Of 12 girls (ages 9-16) with severe and longstanding hypothyroidism, nine were diagnosed by pelvic ultrasound with PCOS. The cysts resolved rapidly after treatment with thyroid hormone. In another study of hypothyroid patients with PCOS, administration of thyroid hormone was associated with normalization of ovulation.23 These observations raise the possibility that sublaboratory hypothyroidism is a contributing factor in some cases of PCOS.”
Lindsay AN, Voorhess ML, MacGillivray MH. Multicystic ovaries in primary hypothyroidism.Obstet Gynecol 1983;61:433-437. 23.
Ghosh S, Kabir SN, Pakrashi A, et al. Subclinicalhypothyroidism: a determinant of polycystic ovary syndrome.
Iodine and PCOS
(33) http://www.optimox.com/pics/Iodine/pdfs/IOD02.pdf
Orthoiodosupplementation: Iodine sufficiency of the whole human Guy. E. Abraham M.D.1, Jorge D. Flechas M.D.2 and John C. Hakala R.Ph.Our preliminary experience with I supplementation at 12.5 mg/day. Our findings in 3 patients with Polycystic Ovarian Syndrome (PCOS) confirmed the positive response observed following supplementation with 10 to 20 mg of potassium iodide by Russian investigators 40 years ago (62). Prior to I supplementation, those PCOS patients were olygomenorrheic, menstruating one or twice a year. Following I supplementation for 3 months, they resumed normal monthly cycles.
(34) http://optimox.com/pics/Iodine/opt_Research_I.shtml
Listing of Iodine publications at the Optimox Web Site.
(35) http://optimox.com/pics/Iodine/IOD-10/IOD_10.htm
Orthoiodosupplementation in a Primary Care Practice Jorge D. Flechas, M.D.
Iodine deficiency may cause the ovaries to develop cysts , nodules and scar tissue. At its worse this ovarian pathology is very similar to that of polycystic ovarian syndrome (PCOS). As of the writing of this article I have five PCOS patients. The patients have successfully been brought under control with the use of 50 mg of iodine per day. Control with these patients meaning cysts are gone, periods every 28 days and type 2 diabetes mellitus under control.
(36) http://cypress.he.net/~bigmacnc/drflechas/index.htm
HelpMyThyroid, George Flechas MD web site
Vitamin D and PCOS
(37) http://www.ncbi.nlm.nih.gov/pubmed/17177140
Low serum 25-hydroxyvitamin D concentrations are associated with insulin resistance and obesity in women with polycystic ovary syndrome. Exp Clin Endocrinol Diabetes. 2006 Nov;114(10):577-83. Hahn S et al. Insulin resistance (IR) and central obesity are common features of the polycystic ovary syndrome (PCOS). Vitamin D is thought to play a role in the pathogenesis of type 2 diabetes by affecting insulin metabolism. Subgroup analysis of lean, overweight and obese women revealed significant higher 25-OH-VD levels in lean women. Differences remained significant when women were divided according to their 25-OH-VD levels. Women with hypovitaminosis D (<9 ng/ml) had higher mean BMI, indices of IR and leptin levels compared to women with normal serum levels (all p<0.05). Analysis of vitamin D and biochemical endocrine PCOS features revealed a significant correlation only between 25-OH-VD and sex hormone-binding globulin as well as the free androgen index. In conclusion, in PCOS women, low 25-OH-VD levels are associated with obesity and insulin resistance .
(38) http://www.ncbi.nlm.nih.gov/pubmed/10433180
Vitamin D and calcium dysregulation in the polycystic ovarian syndrome.Thys-Jacobs S, Donovan D, Papadopoulos A, Sarrel P, Bilezikian JP. Department of Medicine, St. Lukes-Roosevelt Hospital Center, Columbia University, College of Physicians & Surgeons, New York, NY 10019, USA. Steroids. 1999 Jun;64(6):430-5.
Over the past 30 years, numerous studies in invertebrates and vertebrates have established a role of calcium in oocyte maturation as well as in the resumption and progression of follicular development. Polycystic ovarian syndrome (PCO) is characterized by hyperandrogenic chronic anovulation, theca cell hyperplasia, and arrested follicular development. The aim of this observational study was to determine whether vitamin D and calcium dysregulation contribute to the development of follicular arrest in women with PCO, resulting in reproductive and menstrual dysfunction. Thirteen premenopausal women (mean age 31 +/- 7.9 years) with documented chronic anovulation and hyperandrogenism were evaluated. Four women were amenorrheic and nine had a history oligomenorrhea, two of whom had dysfunctional bleeding. Nine had abnormal pelvic sonograms with multiple ovarian follicular cysts. All were hirsute, two had alopecia, and five had acanthosis nigricans. The mean 25 hydrovitamin D was 11.2 +/- 6.9 ng/ml [normal (nl): 9-52], and the mean 1,25 dihydroxyvitamin D was 45.8 +/- 18 pg/ml. with one woman with a 1,25 dihydroxyvitamin D <5 pg/ml (nl: 15-60). The mean intact parathyroid hormone level was 47 +/- 19 pg/ml (nl: 10-65), with five women with abnormally elevated parathyroid hormone levels. All were normocalcemic (9.3 +/- 0.4 mg/dl).
Vitamin D repletion with calcium therapy resulted in normalized menstrual cycles within 2 months for seven women, with two experiencing resolution of their dysfunctional bleeding. Two became pregnant, and the other four patients maintained normal menstrual cycles. These data suggest that abnormalities in calcium homeostasis may be responsible, in part, for the arrested follicular development in women with PCO and may contribute to the pathogenesis of PCO.
METFORMIN
(39) http://content.nejm.org/cgi/content/extract/358/1/47
Metformin for the Treatment of the Polycystic Ovary Syndrome John E. Nestler, M.D. N. Engl. J. Med., January 3, 2008; 358(1): 47 – 54.
(39A) http://www.ovarian-cysts-pcos.com/glucophage-metformin-pcos.html
PCOS and Metformin (Glucophage)
Diet and Weight Loss
(40) http://www.ovarian-cysts-pcos.com/pcos-book-res.html
The Natural Diet Solution for PCOS and Infertility Nancy Dunne, ND Bill Slater, MBA
(41) http://www.ovarian-cysts-pcos.com/PCOS-success.html#sec1
PCOS success stories by Nancy Dunne
Conventional Medical Diagnosis and Treatment of PCOS
(42) http://www.amazon.com/Clinical-Gynecologic-Endocrinology-Infertility-Editorial/dp/0781747953
Speroff on PCOS: Clinical Gynecologic Endocrinology and Infertility by Leon Speroff MD p.493
“A question which has puzzled gynecologists and endocrinologists for many years is what causes polycystic ovaries. There is an answer which is appealing in its logic and clinical applicability. The characteristic polycystic ovary emerges when a state of anovulation persists for any length of time” Should you have a sonogram to make the diagnosis of PCOS? “From 8-14% of normal women will demonstrate ultrasonographic findings typical of polycystic ovaries. Ultrasonography as a diagnostic tool for this condition is unnecessary, and we vigorously discourage its use for this purpose.”
(43) http://assets.cambridge.org/97805218/48497/excerpt/9780521848497_excerpt.pdf
Exerpt from Book: Introduction: Polycystic ovary syndrome is an intergenerational problem. Gabor T. Kovacs and Robert Norman Cambridge University Press 978-0-521-84849-7 – Polycystic Ovary Syndrome, Second Edition
(44) http://findarticles.com/p/articles/mi_qa3890/is_200407/ai_n9457295/pg_1
Hoyt, Karri Lynn “Polycystic Ovary (Stein-Leventhal) Syndrome: Etiology, Complications, and Treatment”. Clinical Laboratory Science. Summer 2004.
(45) http://health.nytimes.com/health/guides/disease/polycystic-ovary-disease/overview.html
Polycystic Ovary Disease article in the New York Times
(46) http://www.ebmonline.org/cgi/content/full/229/5/369
MINIREVIEW, Screening for and Treatment of Polycystic Ovary Syndrome in Teenagers.
Experimental Biology and Medicine 229:369-377 (2004) Darren J. Salmi et al.
(47) http://www.drgalen.com/pcos.html
Dr. Galen, Reproductive Science Centerª of the San Francisco Bay Area, POLYCYSTIC OVARY SYNDROME (PCOS) Treatment of PCOS: In cases where ovulation is irregular or absent, medication can be used. The most common agent is clomiphene citrate (Clomid, Serophene), which is generally taken daily from days 3-7 of a cycle. Ovarian follicle development is usually monitored with a combination of home urinary LH testing, and office ultrasound examination. An intrauterine insemination is frequently advised because of clomiphene’s adverse effect on a womanÕs cervical mucous quality. Additional endometrial support may be promoted with the use of progesterone or HCG injections. There is a mildly increased rate of multiple pregnancy with clomiphene (6-7%) but there is no increased risk of birth defects. The majority of womn who conceive on clomiphene will do so in the first 4 cycles. If clomiphene fails to successfully induce ovulation and/or pregnancy, then a group of injectable hormone preparations, known as gonadotropins, may be employed.
(48) http://www.clinmedres.org/cgi/content/full/2/1/13
Clinical Medicine & Research Volume 2, Number 1 : 13 -27, 2004, Polycystic Ovarian Syndrome: Diagnosis and Management Michael T. Sheehan, MD. Marshfield Clinic. Excellent review of conventional diagnosis and treatment for PCOS.
(49) http://www.inciid.org/printpage.php?cat=pcos&id=505
Understanding and managing Polycystic Ovarian Syndrome (PCOS) by Sam Thatcher, M.D., Ph.D. director of the Center for Applied Reproductive Science in Johnson City, TN,. Conventional Approach.
(50) http://www.perspectivespress.com/0-944934-25-0.html
PCOS: The Hidden Epidemic. a Book by Sam Thatcher MD PhD, Conventional Approach to PCOS.
(51) http://www.emedicine.com/ped/topic2155.htm
Polycystic Ovarian Syndrome Last Updated: September 15, 2006, on E-Medicine.
(52) http://www.endotext.org/female/female6/female6.htm
ENDOTEXT.COM, HYPERANDROGENISM, HIRSUTISM AND POLYCYSTIC OVARY SYNDROMEChapter 6 – Randall B. Barnes, M.D., Adrienne B. Neithardt, M.D. and Suleena K. Kalra, M.D.November 19, 2003 on Endotext.com
(53) http://jcem.endojournals.org/cgi/content/full/89/2/453
EXTENSIVE PERSONAL EXPERIENCE Androgen Excess in Women: Experience with Over 1000 Consecutive Patients R. AZZIZ, L. A. SANCHEZ, E. S. KNOCHENHAUER, C. MORAN, J. LAZENBY, K. C. STEPHENS,K. TAYLOR, AND L. R. BOOTS The Journal of Clinical Endocrinology & Metabolism 89(2):453–462. All patients with menstrual or ovulatory dysfunction received BCPs’ (OCs) when possible. Patients with unwanted hair growth and evidence of excess facial or body terminal hair growth received spironolactone (SPA) (200 mg ; 100 mg/d) in combination with the OC, to minimize the risks of teratogenicity. SPA was rarely used alone, except in the occasional hirsute patient who had previously undergone a hysterectomy or tubal ligation. Other treatment regimens were occasionally used, including glucocorticoids, insulin sensitizers, GnRH analogs, flutamide, finasteride, and other estrogen-progestin combinations, alone or in combination; the majority of these were used as part of clinical trials (24–26).
(54) http://www.joplink.net/prev/200201/ref/01-02.html
Stein IF, Leventhal ML. Amenorrhoea associated with bilateral polycystic ovaries. Am J Obstet Gynecol 1935;29:181–91.
The Environment, Endocrine Disruptor Chemicals and PCOS
(55) http://www.ourstolenfuture.org/Consensus/2005/2005-1030vallombrosa.htm
Vallombrosa Consensus Statement on Environmental contaminants and human fertility compromise.
October 2005.
(56) http://www.ourstolenfuture.org/index.htm
Our Stolen Future, endocrine disruptors in the environment
(57) http://www.ovarian-cysts-pcos.com/news13-pcos-pesticides.html#sec1
Pesticides and PCOS
(58) http://humupd.oxfordjournals.org/cgi/reprint/7/3/323.pdf
Endocrine Disruptors as environmental cause of PCOSThe impact of Endocrine Disruptors on the Female Reproductive System, Stamati and pitsos et al.
Testosterone for Women
(59) http://www.asrm.org/Literature/Menopausal_Medicine/menomedsummer01.pdf
Testosterone Treatment: Psychological and Physical Effects in Postmenopausal Women.
Susan R. Davis, M.B.B.S., F.R.A.C.P., Ph.D. Menopausal Volume 9, Number 2, Summer 2001
Diet for PCOS
(61) http://pcos.is/files/pcosbook1.pdf
A complete online book on Diet and Nutrition for PCOS by Nancy Dunn
(62) http://www.topfitonline.com/chartglycemic.htm
Glycemic Index Chart – handy and useful.
Questionnaire for PCOS
(63) http://www.cfp.ca/cgi/content/full/53/6/1041/T50531041
Table 5 Clinical tool for diagnosis of polycystic ovary syndrome
Can Fam Physician Vol. 53, No. 6, June 2007, pp.1041 – 1047 , Polycystic ovary syndrome. Validated questionnaire for use in diagnosis, Sue D. Pedersen, et al.
(64) http://www.pubmedcentral.nih.gov/articlerender.fcgi?tool=pmcentrez&artid=1949220
Can Fam Physician. 2007 June; 53(6): 1041–1047. Polycystic ovary syndrome. Validated questionnaire for use in diagnosis, Sue D. Pedersen, et al.
(65)http://www.acamnet.org/site/c.ltJWJ4MPIwE/b.2242497/k.2C78/Integrative_Medicine_
Physicians/apps/kb/cs/contactsearch.asp
ACAM doctor’s directory
(66) http://www.worldhealth.net/pages/directory
A4M doctor’s directory
(67) http://jeffreydach.com/2008/02/27/a-commonly-missed-cause-of-infertility-nonclassical-cah-by-jeffrey-dach-md.aspx A Commonly Missed Cause of Infertility, NonClassical CAH by Jeffrey Dach MD
Non Classical Adrenal Hyperplasia CAH 21-OH Deficiency
(68) http://jcem.endojournals.org/cgi/content-nw/full/91/11/4205/F8
FIG. 8. Non-classical CAH 21 Hydroxylase Deficiency Chart of Disease frequencies in different ethnic groups.
(69) http://jcem.endojournals.org/cgi/content/full/91/11/4205
The Journal of Clinical Endocrinology & Metabolism Vol. 91, No. 11 4205-4214
EXTENSIVE CLINICAL EXPERIENCE, Nonclassical 21-Hydroxylase Deficiency
Maria I. New Department of Pediatrics, Mount Sinai School of Medicine, New York, New York 10029
(70) http://www.mcg.edu/pediatrics/pedsendo/21.pdf
Consensus Statement on Treatment of 21-Hydroxylase Deficiency. JCEM 87(9):4048-4053, 2002.
(71) http://www.questdiagnostics.com/hcp/intguide/EndoMetab/Gen_Misc/TG_CAH/TG_CAH_Fig1.pdf
Chart showing pathways of steroid synthsis Quest LAbs.
(72)http://jcem.endojournals.org/cgi/content/full/91/11/4205/F5
FIG. 5. Nomogram relating baseline to ACTH-stimulated serum concentrations of 17-OHP. The scales are logarithmic. A regression line for all data points is shown.
(73)
http://www.questdiagnostics.com/hcp/intguide/jsp/showintguidepage.jsp?fn=EndoMetab/Gen_Misc/TG_CAH/TG_CAH.htm
Congenital Adrenal Hyperplasia Testing Algorithm Guide Quest LAbs
(74) http://www.questdiagnostics.com/hcp/intguide/EndoMetab/EndoManual_AtoZ_PDFs/CAH_Common.pdf
21 Hydroxylase Deficiency Common Mutations, Quest LAbs
(75) http://www.esoterix.com/files/ss_cah.pdf
DNA TESTING FOR 21-HYDROXYLASE DEFICIENCY, Esoterix introduces a new DNA test to identify deficiency in the 21-hydroxylase gene, the most common cause of congenital adrenal hyperplasia (CAH). CAHDetx evaluates the CYP21 gene, detecting mutations and gene deletion/conversions that account for approximately 90% to 95% of all CAH cases.
(76) http://jcem.endojournals.org/cgi/content-nw/full/91/11/4205/T1
TABLE 1. Common gene mutations of the 21-hydroxylase gene CYP21A2 (75 )
(77) http://www.amazon.com/review/R2IPB7XGMO20NE/ref=cm_cr_rdp_perm
Safe Use of Cortisol is a Unique Medical Classic, December 7, 2007 By Jeffrey Dach MD
(78)
http://jeffreydach.com/2008/02/27/a-commonly-missed-cause-of-infertility-nonclassical-cah-by-jeffrey-dach-md.aspx
A Commonly Missed Cause of Infertility, NonClassical CAH by Jeffrey Dach MD
(C) 2008-2013 All Rights Reserved Jeffrey Dach MD Disclaimer
Link to this article: http://wp.me/P3gFbV-7p
Link to this article: http://jeffreydach.com/2008/02/13/understanding-pcos-the-hidden-epidemic-by-jeffrey-dach-md.aspx
disclaimer http://www.drdach.com/wst_page20.html
Disclaimer: The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physicia. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur. Finally, permission is granted to copy or reproduce this article on the internet, provided that appropriate credit and a link to the original article is provided.
This article is Part One of a series,
For Part Two, Click Here.
Images










Jennifla January 5, 2015 at 2:59 PM
The links in this sentence are bad
“If you have PCOS and need a doctor to prescribe progesterone, you can find a knowledgeable physician on the ACAM or A4M doctor’s directory.”
I am in need of an MD who can help with hypothyroidism, PCOS, and cystic breasts. Can someone point me to a directory of MD’s willing to prescribe progesterone cream.