954-792-4663
by Jeffrey Dach MD
The Allan Smith Story – TV Documentary
Allan Smith, a New Zealand Dairy farmer, contracted Swine Flu while away on vacation in Fiji. When he returned home, the flu quickly evolved into severe pneumonia which left him in a coma on Life Support in the Intensive Care Unit. Chest Xrays showed the lungs were completely filled with fluid with an “opaque” appearance called “white out”. After three weeks of this, Allan’s doctors asked the family permission to turn off the machines and let him die. Allan’s wife Sonia had a brother with some medical knowledge, so he stepped in and said, “you haven’t tried everything, You have got to try high dose IV vitamin C on Allan”. At first, the doctors resisted, saying it was useless. Next, the three sons weighed in with a persuasive argument to try the IV vitamin C, saying there was nothing to lose.
Above Left image: IV Bag with Vitamin C, Courtesy of wikimedia Commons.
The Doctors were in unanimous agreement that IV Vitamin C would be useless and a waste of time, and that the patient will certainly die. However, one doctor “felt slightly uneasy” with the decision to turn off life support, without first acceding to the family’s wishes, and so they reluctantly agreed to give the IV Vitamin C. Their plan was to give the IV Vitamin C, show it was useless, and then turn off life support.
That day, Allan Smith was given 25 grams of IV Vitamin C in the evening and another 25 grams in the morning. The next day, a CAT scan of the lungs showed improving air flow and a few days later the Chest Xrays showed the lungs were no longer white, indicating air movement. The improvement was dramatic, clear and plain for all to see. However, the doctors denied it was the Vitamin C, and instead, attributed the improvement to “turning patient into a prone position”.
 Another Battle For Vitamin C
Another Battle For Vitamin CSoon after starting the IV vitamin C, Alan could be taken off ECMO life support, and started breathing on his own. However, unexpectedly, a different physician consultant came in, took over the case and stopped the IV vitamin C. Alan Smith’s condition promptly deteriorated. Allan’s wife, Sonia, called a meeting with this new doctor to no avail. The new doctor rolled his eyes, looked up at the ceiling and uttered, “No More Vitamin C “. Not giving up so easily, the three brothers again weighed in, and demanding the IV vitamin C for dad. The three brothers again used their powers of “persuasion”, and the new doctors reluctantly gave in, restarting the life saving IV vitamin C, but only at low doses of one gram a day. The brothers said, “Mucking about with the Vitamin C showed in his fathers health”. “You had to be thick not to see it.”
Left upper image: Vitamin C molecule chemical structure,Courtesy of wikimedia Commons.
Allan’s condition continued to improve and was eventually transferred to a hospital closer to home, still breathing with ventilator assistance. Here, the family had yet another battle with a new doctor who again stopped the IV Vitamin C. This time. the family brought in a lawyer who sent a warning letter to the hospital threatening legal action. The hospital was forced to restart the vitamin C, however, allowing only low dosage. Finally, Allan Smith was able to sit up in bed and take oral liquids. On their own, the family gave dad 6 grams a day of oral vitamin C. This was a highly absorbable form called Lypo-Spheric Vitamin C, from Livon Labs (Dr Thomas Levy).
Allan continued to improve and was discharged home from the hospital. At home, Allan’s neighbor John joked with him, and said, “Allan, you owe me the 15 dollars I paid to have my suit dry cleaned for your funeral, and you bugger, you came back.” They laughed together at the joke.
Video: 60 Minutes New Zealand TV – the Alan Smith Story, recovery from terminal viral pneumonia with high dose IV Vitamin C. Part One.
Watch Part Two of Documentary- Denying the Obvious New Zealand 60 Minutes- Vitamin C Living Proof.
Interviewed in part two was the Principle Advisor to the Health Ministry and Senior Intensive Care Specialist, David Galler, who denied that the intravenous Vitamin C was a contributing factor in the Allan Smith’s recovery. He proclaimed that the recovery could have been just as likely from a “bus driving by” as the high dose Vitamin C . When asked what he would need as proof to that Vitamin C is effective, he replied he would need a randomized controlled trial, such as those for new drug approval funded by a pharmaceutical company.
Apparently Dr Galler is unaware of three double blind placebo controlled studies of IV Vitamin C in critically ill patients in the ICU. These studies were published in Dr. Galler’s own peer reviewed specialty medical literature. (1-5)
These three studies showed reduced mortality and reduced time on ventilators for septic and critically ill patients in the ICU setting. In addition, numerous other studies have measured blood vitamin C levels in critically ill patients in the hospital showing Vitamin C is typically depleted with levels below 25 % of healthy individuals.(6-11) As Dr Levy points out in Part Four of the Series (see below), there are thousands of studies over 70 years in the medical literature showing effectiveness, and safety of Vitamin C for viral illness. Dr Levy’s book, Curing the Incurable: Vitamin C, Infectious Diseases, and Toxins, 3rd Edition cites 1200 such articles supporting the use of Vitamin C.
Below Chart is from Nathens et al , showing serum vitamin C levels in Critically Ill Surgical patients. Red Line shows subnormal Blood Vitamin C values in untreated patients. Green Line shows high normal Blood Vitamin C values in patients treated with IV Vitamin C. Normal range is 0.5 to 2.0 ng/dl. Vitamin C treated patients (green line) had less pulmonary morbidity , less multi-organ failure and less ventilator dependency when compared to untreated patients (red line).
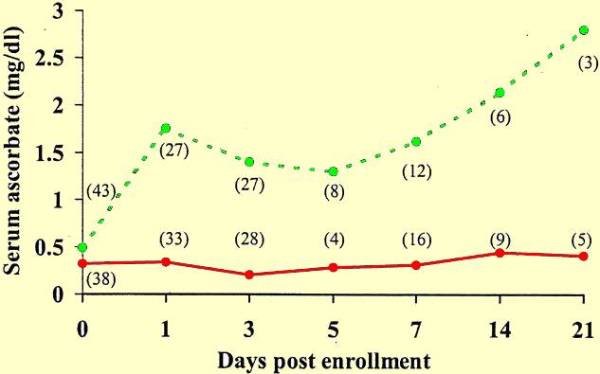 Left chart shows low vitamin C (red line) in Critical care ICU patients, compared to treated patient (green line). Our routine test panel includes a serum vitamin C level for all patients.
Left chart shows low vitamin C (red line) in Critical care ICU patients, compared to treated patient (green line). Our routine test panel includes a serum vitamin C level for all patients.
Dr Galler appeared on New Zealand television claiming to be an authority and medical expert in the care of the ICU critically ill patient. To then make statements amounting to a public admission of ignorance of his own specialty literature is a profound embarrassment to him and to the Ministry of Health that appointed him Advisor. For Allan Smith’s ICU doctors to witness a patient’s dramatic recovery from sure death, and then deny the effectiveness of the treatment is astounding display of denying the obvious, and an embarrassment to the medical system in New Zealand. This is tantamount to holding up a hand in front of a person’s face who then steadfastly denies a hand is in front of his face. It can also be compared to the ridiculous scenario of “denying” that parachutes are lifesaving, and insisting on “proof” by requiring a placebo controlled study. Two men jump out of a plane, one with a parachute and one without a parachute, to “prove” parachutes are effective.
This is a Video interview of Dr Thomas Levy on New Zealand TV – Campbell Live Show. Dr Levy says he was not surprised at the dramatic recovery of Allan Smith from terminal Swine Flu Pneumonia, and he says there is no doubt the Vitamin C was the treatment that saved Allan Smith’s life. Dr Levy sees these types of results regularly from IV Vitamin C and he expects them, just like any well trained doctor would expect prompt recovery from bacterial pneumonia with IV antibiotics.
TV Journalist to Dr Levy: Why do you believe in Vitamin C?
Dr Levy: This is not a belief like its a religion. Data has accumulated over the past 75 years. Studies are published at Harvard and New England Journal. Its amazing that a result is published in a journal and still doesn’t make its way into practice
Experts say we don’t see the proof this is efficacious.
Vitamin C by injection is a registered medicine for treatment of vitamin C deficiency in Zealand. Vitamin C is registered for IV injection.
Where is the evidence it is the kind of cure you say it is?
“I wrote a book, Curing the Incurable: Vitamin C, Infectious Diseases, and Toxins. This book contains 1200 references in the medical literature over the past 85 years, Vitamin C is enormously effective in eradicating infection and toxins.”
Experts say we cannot recommend it. We can find no evidence? Why is this?
I would have to know the motivation because this information is readily available. It’s not information that is hidden, it’s readily available. I would suggest they are closed minded.
I know for a fact by personally using Vitamin C and giving it to my patients and discussions with hundreds of other doctors. What you saw that happened to Allan Smith happens on a regular basis.
How do you know it was vitamin C? Are you singing for your supper? You passionately believe this works.
I passionately know it works. This is not something I have any uncertainly about. If someone treats a dozen patients with pneumococcal pneumonia and they recover, it is the same thing. I’ve seen and done the same thing with Vitamin C.
Buy Buffered Vitamin C from Pure Encapsulations.
Buy Lipospheric Vitamin C on Amazon.
Update 12/16/14:
Fisher, Bernard J, and Ramesh Natarajan. “Phase I Safety Trial of Intravenous Ascorbic Acid in Patients with Severe Sepsis.” Journal of Translational Medicine 12 (2014): 32. PMC. Web. 17 Dec. 2014.
Update Dec 2014
Review: Vitamin C revisited by Heleen M Oudemans-van Straaten*, Angelique ME Spoelstra-de Man and Monique C de Waard Critical Care 2014, 18:460
Published: 6 August 2014
Dr. Suzanne Humphries on Vitamin C:
Links to articles with related content:
MegaDose Vitamins in The ICU by Jeffrey Dach MD
Heart Disease Vitamin C and Linus Pauling by Jeffrey Dach
Dr Fred Klenner
Use _of_Vitamin_C_as_Antibiotic_Fred_Klenner_1953
The Use of Vitamin C as an Antibiotic
Fred R. Klenner, M.D., Reidsville, N.C.
Journal of Applied Nutrition, 1953, Vol. 6, pp. 274–278
Ascorbic_Acid_Fred_klenner_1971
Journal of Applied Nutrition Vol. 23, No’s 3 & 4, Winter 1971
Observations On the Dose and Administration of
Ascorbic Acid When Employed Beyond the Range Of A Vitamin
In Human Pathology Frederick R. Klenner, M.D., F.C.C.P. (1907-1984)
Clinical_Guide_Vitamin_C_Lendon_Smith_2006
Clinical Guide to the Use of Vitamin C,
The Clinical Experiences of Frederick R. Klenner, M.D., summarized by Lendon H. Smith, M.D. 2233 SW Market Street, Portland, Oregon 97201
Update 12/16/14: Dr Suzanne Humphries talks about Vitamin C in Stockholm at Orthomolecular Meeting :
Jeffrey Dach MD
7450 Griffin Road Suite 190
Davie, Florida 33314
954-792-4663
http://www.drdach.com/
http://www.naturalmedicine101.com/
http://www.truemedmd.com/
http://www.bioidenticalhormones101.com/
References:
Vitamin C Benefits Critically Ill, Septic Patients- Three randomized placebo controlled trials.
(1) http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2767105/?tool=pubmed
Biofactors. 2009 Jan–Feb; 35(1): 5–13.
Mechanism of action of vitamin C in sepsis: Ascorbate modulates redox signaling in endothelium John X. Wilson
Subnormal ascorbate concentrations in plasma and leukocytes are common features of the critically ill in general and of patients with sepsis in particular [19–25]. Furthermore, plasma ascorbate correlates inversely with multiple organ failure [19] and directly with survival [21].
Parenteral administration of ascorbate may decrease morbidity and mortality in critically ill patients who are septic or at risk of becoming septic. In a randomized, double-blind, placebo-controlled trial with 216 critically ill patients, 28-day mortality was decreased in the patients who received combined ascorbate and vitamin E by intravenous infusion compared with those who did not [48]. A second randomized trial with 595 critically ill surgical patients found that a combination of ascorbate (1,000 mg q8h by intravenous injection) and vitamin E (1,000 IU q8h by naso- or orogastric tube), begun within 24 h of traumatic injury or major surgery, decreased relative risk of pulmonary edema and multiple organ failure [49]. These two trials were not designed to distinguish between the actions of ascorbate and vitamin E. However, a third randomized trial observed decreased morbidity for severely burned patients who received a very high dose of ascorbate (1,584 mg/kg/day) parenterally [50]. Of particular relevance to microvascular barrier function, ascorbate treatment was associated with significant reductions in edema formation, fluid resuscitation volume, and respiratory dysfunction [50].
2) http://www.ncbi.nlm.nih.gov/pubmed/15333422
Beneficial_Effects_Antioxidant_Supplementation_2004_Anesth_Analg_CrimiThe Beneficial Effects of Antioxidant Supplementation in Enteral Feeding in Critically Ill Patients: A Prospective, Randomized, Double-Blind, Placebo-Controlled Trial. Anesth Analg. 2004 Sep;99(3):857-63. Ettore Crimi, MD*, Antonio Liguori, MD†, Mario Condorelli, MD‡, Michele Cioffi, MD§, Marinella Astuto, MD∥, Paola Bontempo, MD PhD§, Orlando Pignalosa, MD§, Maria Teresa Vietri, MD§, Anna Maria Molinari, MD§, Vincenzo Sica, MD§, Francesco Della Corte, MD* and Claudio Napoli, MD PhD
Department of Anesthesiology and Intensive Care, University of Eastern Piedmont, Novara, Italy;†Coronary Care Unit, Pellegrini Hospital, Naples, Italy; ‡Department of Medicine, University of Naples, Naples, Italy; §Division of Clinical Pathology, II University of Naples, Naples, Italy; and ∥Department of Anesthesiology and Intensive Care, University of Catania, Catania, Italy
We investigated whether intervention with antioxidant vitamins C and E in enteral feeding influenced oxidative stress and clinical outcome in critically ill patients. Two-hundred-sixteen patients expected to require at least 10 days of enteral feeding completed the study. One-hundred-five patients received enteral feeding supplemented with antioxidants, and 111 control patients received an isocaloric formula. Plasma lipoperoxidation (by thiobarbituric acid reactive substances [TBARS] and prostaglandin F2α isoprostane levels), low-density lipoprotein (LDL) oxidizability, and LDL tocopherol content were determined at baseline and at the end of the 10-day period. The clinical 28-day outcome was also assessed. Plasma TBARS and isoprostanes were 5.33 ± 1.26 nM/mL and 312 ± 68 pg/mL, respectively, before treatment and 2.42 ± 0.61 nM/mL and 198 ± 42 pg/mL after intervention (P < 0.01 for both comparisons). Antioxidants improved LDL resistance to oxidative stress by approximately 30% (the lag time before treatment was 87 ± 23 min and was 118 ± 20 min after treatment; P < 0.04). There was a significantly reduced 28-day mortality after antioxidant intervention (45.7% in the antioxidant group and 67.5% in the regular-feeding group; P < 0.05). Isoprostanes may provide a sensitive biochemical marker for dose selection in studies involving antioxidants.
In summary, we show that AOX intervention with proper doses of vitamin E and C supplemental to enteral feeding prevents lipid peroxidation and oxidative stress in vivo. AOX intervention also significantly influenced the 28-day outcome in critically ill patients. In absolute terms, mortality was frequent, but this was expected because this condition is relatively common in elderly patients with frequent comorbidities (28,29). Among patients older than 65 years of age, Knaus et al. (28) reported hospital mortality rates of 60% with 1 organ system failure, 90% with 2 organ system failures, and 100% with 3 or more organ system failures.
Our findings are in agreement with those of a large clinical study (595 patients) showing that AOX supplementation reduces the incidence of organ failure and shortens the length of stay in a cohort of critically ill surgical patients (30). The lack of adverse effects, coupled with the minimal expense, supports the use of AOX in critically ill patients. Interestingly, there is growing interest in superoxide dismutase mimetics in critical care medicine (31).
(3) http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1422648/?tool=pubmed
Ann Surg. 2002 Dec;236(6):814-22.
Randomized, prospective trial of antioxidant supplementation in critically ill surgical patients. Nathens AB, Neff MJ, Jurkovich GJ, Klotz P, Farver K, Ruzinski JT, Radella F, Garcia I, Maier RV. Division of Trauma and General Surgery, Harborview Medical Center and the Department of Surgery, University of Washington, Seattle, Washington, USA.
Abstract
OBJECTIVE: To determine the effectiveness of early, routine antioxidant supplementation using alpha-tocopherol and ascorbic acid in reducing the rate of pulmonary morbidity and organ dysfunction in critically ill surgical patients.
SUMMARY BACKGROUND DATA: Oxidative stress has been associated with the development of the acute respiratory distress syndrome (ARDS) and organ failure through direct tissue injury and activation of genes integral to the inflammatory response. In addition, depletion of endogenous antioxidants has been associated with an increased risk of nosocomial infections. The authors postulated that antioxidant supplementation in critically ill surgical patients may reduce the incidence of ARDS, pneumonia, and organ dysfunction.
METHODS: This randomized, prospective study was conducted to compare outcomes in patients receiving antioxidant supplementation (alpha-tocopherol and ascorbate) versus those receiving standard care. The primary endpoint for analysis was pulmonary morbidity (a composite measure of ARDS and nosocomial pneumonia). Secondary endpoints included the development of multiple organ failure, duration of mechanical ventilation, length of ICU stay, and mortality.
RESULTS: Five hundred ninety-five patients were enrolled and analyzed, 91% of whom were victims of trauma. The relative risk of pulmonary morbidity was 0.81 (95% confidence interval 0.60-1.1) in patients receiving antioxidant supplementation. Multiple organ failure was significantly less likely to occur in patients receiving antioxidants than in patients receiving standard care, with a relative risk of 0.43 (95% confidence interval 0.19-0.96). Patients randomized to antioxidant supplementation also had a shorter duration of mechanical ventilation and length of ICU stay.
CONCLUSIONS: The early administration of antioxidant supplementation using alpha-tocopherol and ascorbic acid reduces the incidence of organ failure and shortens ICU length of stay in this cohort of critically ill surgical patients.
Following treatment assignment, patients randomized to antioxidant supplementation received α-tocopherol (dl-α-tocopheryl acetate; Aquasol E, Astra USA, Westborough, MA) 1,000 IU (20 mL) q8h per naso- or orogastric tube and 1,000 mg ascorbic acid given intravenously (American Reagent Labs, Shirley, NY) in 100 mL D5W q8h for the shorter of the duration of admission to the ICU or 28 days.
(4) http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2575590/?tool=pubmedCrit Care. 2008; 12(4): R101.
Published online 2008 August 7. doi: 10.1186/cc6981. PMCID: PMC2575590
Influence of early antioxidant supplements on clinical evolution and organ function in critically ill cardiac surgery, major trauma, and subarachnoid hemorrhage patients
Mette M Berger,1 Ludivine Soguel,1 Alan Shenkin,2 Jean-Pierre Revelly,1 Christophe Pinget,3 Malcolm Baines,2 and René L Chioléro1
The intervention was intravenous supplements for 5 days (selenium 270 μg, zinc 30 mg, vitamin C 1.1 g, and vitamin B1 100 mg) with a double-loading dose on days 1 and 2 or placebo.
ICU Study on ventilator dependency
(5) http://www.ncbi.nlm.nih.gov/pubmed/20149369
Injury. 2010 Jul;41(7):857-61. Epub 2010 Feb 10.
High-dose antioxidant administration is associated with a reduction in post-injury complications in critically ill trauma patients. Giladi AM, Dossett LA, Fleming SB, Abumrad NN, Cotton BA. Department of Surgery, University of Michigan, Ann Arbor, MI, United States. Abstract BACKGROUND: We recently demonstrated a high-dose antioxidant (AO) protocol was associated with reduction in mortality. The purpose of this study was to evaluate the impact of AO on organ dysfunction and infectious complications following injury.
PATIENTS AND METHODS: High-dose AO protocol: ascorbic acid 1000 mg q 8 h, alpha-tocopherol 1000 IU q 8 h, and selenium 200 mcg qd for 7-day course. Retrospective cohort study evaluating all patients admitted after protocol implementation (AO+), October 1, 2005 to September 30, 2006. Comparison cohort (AO-): all patients admitted in the year prior to implementation, October 1, 2004 to September 30, 2005.
RESULTS: 2272 patients included in the AO+ group, 2022 patients in the AO- group. Demographics and injury severity were similar. Abdominal compartment syndrome (ACS) (2.9% vs. 0.7%, <0.001), surgical site infections (2.7% vs. 1.3%, p=0.002), pulmonary failure (27.6% vs. 17.4%, p<0.001), and ventilator-dependent respiratory failure (10.8% vs. 7.1%, p<0.001) were significantly less in the AO+ group. Multivariate regression showed 53% odds reduction in abdominal wall complications and 38% odds reduction in respiratory failure in the AO+ group.
CONCLUSIONS: Implementation of a high-dose AO protocol was associated with a reduction in respiratory failure and ventilator-dependence. In addition, AO were associated with a marked decrease in abdominal wall complications, including ACS and surgical site infections.
(6) http://www.ajcn.org/cgi/reprint/63/5/760.pdf
Am J Clin Nutr. 1996 May;63(5):760-5.
Total vitamin C, ascorbic acid, and dehydroascorbic acid concentrations in plasma of critically ill patients. Schorah CJ, Downing C, Piripitsi A, Gallivan L, Al-Hazaa AH, Sanderson MJ, Bodenham A. Division of Clinical Sciences, University of Leeds, United Kingdom.
Abstract
Plasma concentrations of the antioxidant vitamin ascorbic acid were measured by high-performance liquid chromatography in critically ill patients in whom the excessive generation of reactive oxygen species could compromise antioxidant defense mechanisms. Median concentrations of both total vitamin C (ascorbic acid and dehydroascorbic acid) and ascorbic acid in these patients were < 25% (P < 0.001) of the values found in healthy control subjects and in subjects in two other disease groups (diabetes, gastritis) in which reactive oxygen species are reported to be increased. The low values could not be explained by age, sex, intake, or treatment differences, but were associated with the severity of the illness and were not prevented by the use of parenteral nutrition containing ascorbic acid. In addition, the vitamin was less stable in blood samples taken from critically ill patients than in similar samples from subjects in the other groups. The findings indicate that antioxidant defenses could be considerably compromised in these very sick patients. If this reduces the patient’s capacity to scavenge reactive species, then the potential of these species to damage DNA and lipid membranes could be increased and compromise recovery.
(7) http://www.journalofsurgicalresearch.com/article/S0022-4804(02)00083-5/abstract
JSR Volume 109, Issue 2, Pages 144-148 (February 2003) Ascorbic acid dynamics in the seriously ill and injured C.L Long, Ph.D., K.I Maull, M.D., R.S Krishnan, M.D., H.L Laws, M.D., J.W Geiger, B.S., L Borghesi, M.D., W Franks, R.Ph., MBA†, T.C Lawson, M.D., H.E Sauberlich, Ph.D.† Received 3 July 2002
Abstract Background. In addition to the known beneficial effects of ascorbic acid on wound healing and the immune response, it is also a potent extracellular antioxidant. Recent work in septic rats suggests that high-dose ascorbic acid total parenteral nutrition (TPN) supplementation may protect cells from free radical injury and improve survival. In this study, we determined ascorbic acid levels in the immediate post-injury/illness period and evaluated the ability of early short-term high levels of ascorbic acid in TPN to normalize plasma levels.
Materials and Methods. Ascorbic acid levels were determined in 12 critically injured patients and 2 patients with severe surgical infections. Each patient received TPN supplemented with increasing doses of ascorbic acid over a 6-day period. Therapeutic responses were determined by plasma and urine measurements using high-pressure liquid chromatography.
Results. The initial mean ± SEM baseline plasma ascorbic acid concentration was depressed (0.11 ± 0.03 mg/dl) and unresponsive following 2 days on 300 mg/day supplementation (0.14 ± 0.03; P = 1.0) and only approached low normal plasma levels following 2 days on 1000 mg/day (0.32 ± 0.08; P = 0.36). A significant increase was noted following 2 days on 3000 mg/day (1.2 ± 0.03; P = 0.005).
Conclusion. We confirmed extremely low plasma levels of ascorbic acid following trauma and infection. Maximal early repletion of this vitamin requires rapid pool filling early in the post-injury period using supraphysiologic doses for 3 or more days.
(8) http://www.ncbi.nlm.nih.gov/pubmed/20689415
Current Opinion in Clinical Nutrition & Metabolic Care:
Vitamin C requirement in surgical patients Fukushima, Ryoji; Yamazaki, Eriko
Recent findings: Blood vitamin C concentration falls after uncomplicated surgery and further decreases in surgical intensive care unit patients. The decline may be owing to increased demand caused by increased oxidative stress. To normalize plasma vitamin C concentration, much higher doses than the recommended daily allowance or doses recommended in parenteral nutrition guidelines are needed in these patients. In uncomplicated surgical patients, more than 500 mg/day of vitamin C may be required, with much higher doses in surgical intensive care unit patients. In uncomplicated gastrointestinal surgery, continuous parenteral administration of 500 mg/day of vitamin C reduced postoperative oxidative stress as manifested by reduced urinary excretion of isoprostane. In some studies, postoperative atrial fibrillation was prevented after cardiac surgery by perioperative vitamin C supplementation. In critically ill patients, some prospective randomized controlled trials support parenteral supplementation of high doses of vitamin C, E and trace elements.Summary: Vitamin C requirement is increased in surgical patients, and the potential advantage of supplementation is to increase the plasma and tissue levels of vitamin C and thereby reduce oxidative stress. Although some clinical benefits of high-dose vitamin C supplementation have been shown in the critically ill, the optimal dose for supplementation and the clinical benefits remain to be investigated in surgical patients.
Low Vitamin C levels in Hospitalized patients
(9) http://www.ncbi.nlm.nih.gov/pubmed/20018480
Nutrition. 2009 Dec 15. [Epub ahead of print]
Metabolic origin of hypovitaminosis C in acutely hospitalized patients. Evans-Olders R, Eintracht S, John Hoffer L. Lady Davis Institute for Medical Research, McGill University and Jewish General Hospital, Montreal, Quebec, Canada.
RESULTS: Vitamin C administration increased plasma and mononuclear leukocyte vitamin C concentrations from subnormal (16.3 +/- 12.4 mumol/L and 6.5 +/- 5.5 mmol/L, respectively) to normal (71.0 +/- 30.9 mumol/L, P < 0.0001, and 8.2 +/- 6.8 mmol/L, P < 0.015); the mood disturbance score improved by 33% (P < 0.008). There was no increase in plasma glutathione concentrations or a reduction in plasma or mononuclear leukocyte malondialdehyde concentrations. An inverse relation was observed between plasma C-reactive protein and plasma vitamin C concentrations (P = 0.006).
(10) http://www.ncbi.nlm.nih.gov/pubmed/14614974
Eur J Intern Med. 2003 Nov;14(7):419-425. Hypovitaminosis C in hospitalized patients.
Fain O, Pariés J, Jacquart B, Le Moël G, Kettaneh A, Stirnemann J, Héron C, Sitbon M, Taleb C, Letellier E, Bétari B, Gattegno L, Thomas M.
RESULTS: The prevalence of hypovitaminosis C (depletion: SAAL<5 mg/l or deficiency: SAAL<2 mg/l ) was 47.3%. Some 16.9% of the patients had vitamin C deficiency. There was a strong association between hypovitaminosis C and the presence of an acute phase response (p=0.002). Other univariate risk factors for vitamin C depletion were male sex (p=0.02), being retired (p=0.037), and infectious diseases (p=0.002). For vitamin C deficiency, the significant univariate risk factors included the same ones found for vitamin C depletion, plus being unemployed (p=0.003) and concomitant excessive alcohol and tobacco consumption (p<0.0001). Logistic regression showed that being retired (p=0.015) and concomitant excessive alcohol and tobacco consumption (p=0.0003) were significant independent risk factors. Hemorrhagic syndrome and edema were described more often in patients with vitamin C deficiency than in those with vitamin C depletion or without hypovitaminosis. Clinical signs were more frequent for an ascorbic acid level below 2.5 mg/l.
CONCLUSION: Hypovitaminosis C is frequent in hospitalized patients but should be interpreted according to the presence or absence of an acute phase response. The main risk factors are living conditions and excessive alcohol and tobacco consumption.
(11) http://www.jacn.org/cgi/content/abstract/27/3/428
Journal of the American College of Nutrition, Vol. 27, No. 3, 428-433 (2008)
Published by the American College of Nutrition Vitamin C Deficiency in a University Teaching Hospital Runye Gan, Shaun Eintracht, MD and L. John Hoffer, MD, PhD
http://jn.nutrition.org/cgi/content/full/136/10/2611
2006 American Society for Nutrition J. Nutr. 136:2611-2616, October 2006
Nutritional Immunology
Vitamin C Deficiency Increases the Lung Pathology of Influenza Virus–Infected Gulo–/– Mice1
Wei Li2, Nobuyo Maeda3 and Melinda A. Beck2,*
This study was designed to determine the effects of vitamin C deficiency on the immune response to infection with influenza virus. L-Gulono–lactone oxidase gene-inactivated mice (gulo–/– mice) require vitamin C supplementation for survival. Five-wk-old male and female gulo–/– mice were provided water or water containing 1.67 mmol/L vitamin C for 3 wk before inoculation with influenza A/Bangkok/1/79. There were no differences in lung influenza virus titers between vitamin C–adequate and –deficient mice; however, lung pathology in the vitamin C–deficient mice was greater at 1 and 3 d after infection but less at d 7 compared with vitamin C–adequate mice. Male vitamin C–deficient mice had higher expression of mRNA for regulated upon activation normal T expressed and secreted (RANTES), IL-1ß, and TNF- in the lungs at d 1 after infection compared with male controls. However, at d 3 after infection, male vitamin C–deficient mice had less expression of mRNA for RANTES, monocyte chemotactic protein-1 (MCP-1), and IL-12 compared with male controls. None of these differences were observed in female mice. Vitamin C–deficient male mice also had greater nuclear factor-B activation as early as 1 d after infection compared with male controls. These data suggest that vitamin C is required for an adequate immune response in limiting lung pathology after influenza virus infection.
Dr Fred Klenner
http://www.ltdk.helsinki.fi/users/hemila/CP/Klenner_1948_ch.pdf
http://www.seanet.com/~alexs/ascorbate/194x/
klenner-fr-southern_med_surg-1948-v110-n2-p36.htm
Virus Pneumonia and Its Treatment With Vitamin C . Fred R. Klenner, M.D., Reidsville, North Carolina – Read by Title to the Tri-State Medical Association of the Carolinas and Virginia, meeting at Charleston, February 9th and 10th
http://www.ncbi.nlm.nih.gov/pubmed/18147027
South Med Surg. 1949 Jul;111(7):209-14.
The treatment of poliomyelitis and other virus diseases with vitamin C. KLENNER FR
http://www.seanet.com/~alexs/ascorbate/194x/klenner-fr-southern_med_surg-1949-v111-n7-p209.htm
The Treatment of Poliomyelitis and Other Virus Diseases with Vitamin C
From Southern Medicine & Surgery, Volume 111, Number 7, July, 1949, pp. 209-214
Fred R. Klenner, M.D., Reidsville, North Carolina
http://www.doctoryourself.com/klennerbio.html
HIDDEN IN PLAIN SIGHT: The Pioneering Work of FREDERICK ROBERT KLENNER, M.D.
by Andrew W. Saul Assistant Editor, Journal of Orthomolecular Medicine
J Orthomolecular Med, 2007. Vol 22, No 1, p 31-38.
http://www.seanet.com/~alexs/ascorbate/198x/smith-lh-clinical_guide_1988.htm
Clinical Guide to the Use of Vitamin C The Clinical Experiences of Frederick R. Klenner, M.D.,
abbreviated, sumarized and annotated by Lendon H. Smith, M.D.
2233 SW Market Street, Portland, Oregon 97201
http://www.seleneriverpress.com/media/pdf_docs/
ASCORBIC_ACID_AS_A_CHEMOTHEROPEUTIC_AGENT_-WJ_McCORMICK_RPRNT_5c.pdf
ASCORBIC ACID AS A CHEMOTHERAPEUTIC AGENT W. J. McCormick, M.D.,Toronto, Canada. ARCHIVES OF PEDIATRICS, New York The Practical Monthly on the Diseases of Infants and Children 69: 151-155, April 1952
http://www.orthomolecular.org/library/jom/1991/pdf/1991-v06n02-p099.pdf
The Origin of the 42-Year Stonewall of Vitamin C Robert Landwehr1
http://www.indiaenvironmentportal.org.in/files/Vitamin%20C%20Intravenous%20Use%20by%20Complementary.pdf
Vitamin C: Intravenous Use by Complementary and Alternative Medicine Practitioners and Adverse Effects Sebastian J. Padayatty1., Andrew Y. Sun1., Qi Chen2, Michael Graham Espey1, Jeanne Drisko2, Mark Levine1* 1 Molecular and Clinical Nutrition Section, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, Maryland, United States of America, 2 Program in Integrative Medicine, University of Kansas Medical Center, Kansas City, Kansas, United States of America
http://injectablevitaminc.com/download.html
Injectable Vitamin C, an e-book on the internet by Robert McCracken PhD
http://www.ncbi.nlm.nih.gov/pubmed/17253561
Cochrane Database Syst Rev. 2007 Jan 24;(1):CD005532.
Vitamin C for preventing and treating pneumonia.Hemilä H, Louhiala P.
University of Helsinki, Department of Public Health, POB 41, Mannerheimintie 172, Helsinki, Finland, FIN-00014.
AUTHORS’ CONCLUSIONS: The prophylactic use of vitamin C to prevent pneumonia should be further investigated in populations who have high incidence of pneumonia, especially if dietary vitamin C intake is low. Similarly, the therapeutic effects of vitamin C should be studied especially in patients with low plasma vitamin C levels. The current evidence is too weak to advocate widespread prophylactic use of vitamin C to prevent pneumonia in the general population. However, therapeutic vitamin C supplementation may be reasonable for pneumonia patients who have low vitamin C plasma levels because its cost and risks are low.
Vitamin C Prevents Flu
http://ebm.rsmjournals.com/cgi/content/full/232/7/847
Exp. Biol. Med. 2007;232:847-851 Ascorbic Acid Role in Containment of the World Avian Flu PandemicJohn T. A. Ely1 Radiation Studies, University of Washington, Seattle, Washington 98195 (i) ascorbic acid is not being administered to humans infected or at risk for influenza, and (ii) ascorbic acid is (mistakenly) believed to be a vitamin (“vitamin C”). Proper use of ascorbic acid as described here could provide effective containment for the flu pandemic.
Vitamin C Can Cure – Web Site
http://www.vitaminccancure.org/events
quote: In response to the Auckland DHB 14th September press release, visiting Vitamin C expert, Dr Thomas Levy said today, “to assert that there is ‘no evidence’ that high-dose vitamin C is either safe or effective is to ignore the results of thousands of such IV administrations by doctors around the world, as well as to ignore tens of thousands of articles in the medical literature, in the most esteemed medical institutions in the world, that have been published over the last 70 years.” The DHB decision was made in the wake of mounting demand for high-dose vitamin C after news broke out of Waikato Dairy farmer Alan Smith’s complete recovery from what the hospital classed as a terminal case of Swine flu. Mr Smith is the hospital’s only Swine Flu patient on life support to have survived. He is also the only one to have received the high-dose intravenous vitamin C, which was administered at the family’s request after being advise that life support, and therefore his life, were about to be terminated. Introduced by Alan Smith himself, Dr Levy, cardiologist, associate professor, lawyer and author, spoke about Vitamin C, use, myths, safety and efficacy on Friday 17th September, at Auckland Girls Grammar School, New Zealand. end quote
Thomas Levy MD JD Book Curing the Incurable
http://www.livonlabs.com/cgi-bin/start.cgi/LV/apps/curing-the-incurable.html
http://www.amazon.com/review/R1H1ZW20OC44I7/
Curing the Incurable, Vitamin C, Infectious Disease and Toxins by Thomas E Levy MD JD A Remarkable Medicine Has Been Overlooked, December 15, 2007 By Jeffrey Dach MD
http://www.livonlabs.com/
Lypo-SphericTM Vitamin C proven many times more powerful than all other oral forms of Vitamin C Recent clinical trials by world-renowned Vitamin C expert and pharmacologist, Steve Hickey, PhD, show that Lypo-SphericTM Vitamin C is able to produce serum levels of Vitamin C nearly double those thought theoretically possible with any oral form of Vitamin C.*
1-866-682-6193
LivOn Laboratories
2654 W. Horizon Ridge Pkwy,
Suite B5-108
Henderson, NV 89052
http://www.plosmedicine.org/article/info%3Adoi%2F10.1371%2Fjournal.pmed.0050012
Combined Impact of Health Behaviours and Mortality in Men and Women: The EPIC-Norfolk Prospective Population Study Kay-Tee Khaw1*, Nicholas Wareham2, Sheila Bingham3, Ailsa Welch1, Robert Luben1, Nicholas Day1
population study of 20,244 men and women with no known cardiovascular disease or cancerat baseline survey in 1993–1997, living in the general community in the United Kingdom,and followed up to 2006. Participants scored one point for each health behaviour: currentnon-smoking, not physically inactive, moderate alcohol intake (1–14 units a week)and plasma vitamin C >50 mmol/l indicating fruit and vegetable intake of at least five servings a day, for a total score ranging from zero to four.
Higher Vitamin C Levels mean reduced all cause mortality
http://www.ncbi.nlm.nih.gov/pubmed/11247548
Lancet. 2001 Mar 3;357(9257):657-63.
Relation between plasma ascorbic acid and mortality in men and women in EPIC-Norfolk prospective study: a prospective population study. European Prospective Investigation into Cancer and Nutrition. Khaw KT, Bingham S, Welch A, Luben R, Wareham N, Oakes S, Day N.
Department of Public Health and Primary Care, Institute of Public Health, University of Cambridge School of Clinical Medicine, UK. lasma ascorbic acid concentration was inversely related to mortality from all-causes, and from cardiovascular disease, and ischaemic heart disease in men and women. Risk of mortality in the top ascorbic acid quintile was about half the risk in the lowest quintile (p<0.0001).
http://www.ajcn.org/cgi/content/full/87/1/64
American Journal of Clinical Nutrition, Vol. 87, No. 1, 64-69, January 2008
Plasma vitamin C concentrations predict risk of incident stroke over 10 y in 20 649 participants of the European Prospective Investigation into Cancer–Norfolk prospective population study 1,2,3Phyo K Myint, Robert N Luben, Ailsa A Welch, Sheila A Bingham, Nicholas J Wareham and Kay-Tee Khaw
top quartiles of baseline plasma vitamin C concentrations had a 42% lower risk (relative risk: 0.58; 95% CI: 0.43, 0.78) than did those in the bottom quartile,
http://www.ncbi.nlm.nih.gov/pubmed/10488881?dopt=Abstract
Int J Tuberc Lung Dis. 1999 Sep;3(9):756-61.
Vitamin C and acute respiratory infections. Hemilä H, Douglas RM. Department of Public Health, University of Helsinki, Finland.
Abstract
So far over 60 studies have examined the effects of vitamin C on the common cold. No effect on common cold incidence was observed in the six largest studies, indicating that vitamin C has no preventive effects in normally nourished subjects in the Western countries. There are, however, smaller studies reporting benefit. In three trials of subjects under heavy acute physical stress, common cold incidence decreased by on average 50%, and in four trials of British males common cold incidence decreased by on average 30% in the vitamin C groups. The dietary vitamin C intake in the UK is low, and consequently the benefit may be due to the correction of marginal deficiency, rather than high vitamin doses. Regular vitamin C supplementation (> or =1 g/day) has quite consistently reduced the duration of colds, but the size of the benefit has varied greatly. In the four largest studies the duration of colds was reduced only by 5%. In two of these studies, however, absence from school and work was reduced by 14-21% per episode, which may have practical importance. Three controlled studies recorded a reduction of at least 80% in the incidence of pneumonia in the vitamin C group, and one randomised trial reported substantial treatment benefit from vitamin C in elderly UK patients hospitalized with pneumonia or bronchitis. It seems that the preventive effects of supplementation are mainly limited to subjects with low dietary vitamin C intake, but therapeutic effects may occur in wider population groups. Further carefully designed trials are needed to explore the effects of vitamin C.
http://www.ncbi.nlm.nih.gov/pubmed/10543583?dopt=Abstract
The effectiveness of vitamin C in preventing and relieving the symptoms of virus-induced respiratory infections. Gorton HC, Jarvis K. Abstract
BACKGROUND: An ever increasing demand to evaluate the effect of dietary supplements on specific health conditions by use of a “significant scientific” standard has prompted the publication of this study.
OBJECTIVE: To study the effect of megadose Vitamin C in preventing and relieving cold and flu symptoms in a test group compared with a control group.
DESIGN: Prospective, controlled study of students in a technical training facility.
SUBJECTS: A total of 463 students ranging in age from 18 to 32 years made up the control group. A total of 252 students ranging in age from 18 to 30 years made up the experimental or test group.
METHOD: Investigators tracked the number of reports of cold and flu symptoms among the 1991 test population of the facility compared with the reports of like symptoms among the 1990 control population. Those in the control population reporting symptoms were treated with pain relievers and decongestants, whereas those in the test population reporting symptoms were treated with hourly doses of 1000 mg of Vitamin C for the first 6 hours and then 3 times daily thereafter. Those not reporting symptoms in the test group were also administered 1000-mg doses 3 times daily.
RESULTS: Overall, reported flu and cold symptoms in the test group decreased 85% compared with the control group after the administration of megadose Vitamin C.
CONCLUSION: Vitamin C in megadoses administered before or after the appearance of cold and flu symptoms relieved and prevented the symptoms in the test population compared with the control group.
Allan Smith Story from Brad Weeks MD
http://weeksmd.com/?p=4191
Posted by Brad Weeks, MD on September 2, 2010
I want to make it clear that adequately dosed vitamin C, to my knowledge, has never failed to cure an acute viral syndrome. Specifically, all these doctors should now realized that H1N1, the swine flu virus, while perhaps proving to be more potent than a host of other flu viruses, need not be a feared bogeyman with vitamin C in their arsenal.
While I intend to assemble a more substantial case report from the hospital chart in the future, here are the words of my colleague in New Zealand, John Appleton:
“The short story is: Waikato farmer goes to Fiji for holiday, Starts developing flu like symptoms–decides to tough it out Arrives back in NZ very sick–swine flu Tauranga Hospital not able to treat him (what was not known at the time is that he has leukemia–he didn’t know either) Sent him to Auckland Hospital–continues to deteriorate–Tamiflu–antibiotics etc. (usual stuff) Brother-in-law (knows a bit about vitamin C) contacts Thomas Levy in the US who refers him to me I provided a lot of info on vitamin C etc and referred family to CAM (Centre for Advanced Medicine) www.camltd.co.nz in Auckland Family pushes to get him some IVC–hospital refuses CAM doctors encourages hospital then to try vitamin C Patient deteriorates further and is on life support–family told nothing more can be done and life support will be switched off on Monday. Lungs not functioning.
Family says NO–until everything has been tried–they won’t agree to life support being ’switched off’. Hospital is pushed hard to give him IVC and reluctantly they agree. (50 grams twice a day I think) saying if no improvement by Friday that’s it Patient shows signs of improvement by Wednesday–hospital very surprised Concerns expressed about kidneys (which we anticipated) New specialist wants to stop vitamin C–family is told liver is failing ’caused by vitamin C’. I give them lots of data to say liver is more likely to be affected by antibiotics. Patient recovery continues to the point where he can be transferred to Waikato (closer to home); on ventilator and NG tube feeding Doctors there more receptive to vitamin C but won’t agree to continue as per Auckland Family gets (name deleted) high profile lawyer involved who writes letter about patient rights and rings hospital to recommend that they can either sort it out with the family or……? Hospital continues with VC albeit at a much lower dose. CAM doctor travels to Waikato to endorse and recommend IVC at higher doses. I have heard that the lawyer was shocked at what she learned about hospital system
Patient continues to recover–now conscious (thinks he has only been in hospital 3 days)–now 8 weeks in total Hospital staff stunned–never seen anything like this Patient is told by brother-in-law that VC has saved him Family absolutely blown away at what has gone on. Wife has not lost her husband and children have their father.Patient now fully ‘with it’ and is talking normally with family and taking Lypospheric vitamin C (6 grams daily)”
For those doctors wondering about doses, I communicated directly with the brother-in-law. He informed me that on the Tuesday following the initial “deadline” 25 grams was given intravenously. On Wednesday, 25 gram infusions were again repeated twice. Thursday the patient received 75 grams, and starting on Friday he received 100 grams intravenously and stayed at this dose daily for another 4 to 6 days. Then the new consultant had the vitamin C discontinued completely. One week later, the IVC was restarted at only one gram twice daily.
Please resend this case history to any and all who you think could benefit, including your friends and contacts in our government. The latest info on the swine flu indicates it certainly has the potential capacity to become a great killer. This does not have to be the case. Obviously, a reasonable daily dose of vitamin C could be expected to do an even better job at preventing H1N1 while having no downside relative to the mass vaccinations getting ready to take place.
Below find the link to the New Zealand 60 Minutes show on the “terminal” advanced swine flu patient cured with intravenous vitamin C. Also note toward the end of the clip that the patient’s hairy cell leukemia “disappeared” as well. The abilities of properly utilized vitamin C are slowly but surely beginning to be recognized.
http://www.camltd.co.nz/h1n1.html 29 September 2009
The Alan SMith Story from CAM New Zealand
56 year old male was referred to Auckland Hospital ICU on 1 July 2009 with total respiratory failure, for ECMO external oxygenation. The patient had contracted H1N1 Swine flu (confirmed by tests) while on holiday overseas, and had developed what is known as ‘white out’ pneumonia. This refers to x-rays showing no air space in the lungs.
After 20 days of life-sustaining ECMO treatment and other critical care, the patient, who was unconscious by induced coma, had not responded. The ICU team advised the family of the likely outcome and had prepared them for the possibility of the patient’s death.
Family members approached Centre for Advanced Medicine Limited (CAM) for advice on the clinical use of intravenous vitamin C for such cases.
At the family’s request, information was provided to ICU doctors including ISO 9001:2008 registered protocols, safety data, dosages and access to vials of IV vitamin C under CAM’s license for wholesale medicines.
The ICU team agreed to administer intravenous vitamin C according to the family’s wishes. This decision acknowledged the family’s rights, in compliance with the New Zealand Health and Disability Act, 1997.
The patient received intravenous vitamin C starting on the evening of 21 July, continuing until 29 July. 25 grams was provided on the first day increasing over the first three days to 50 grams twice daily which was sustained for a further six days.
By 24 July x-rays indicated increasing lung function and ECMO external oxygenation was discontinued on 26 July. After several days of assisted ventilation and critical care for ongoing secondary conditions, the patient was able to commence his recovery and rehabilitation.
The patient was discharged from hospital on Friday 18 September, and is recovering at home on the farm.
The decision by the Auckland Hospital ICU team to administer adequate dosages of IV vitamin C, and their skillful coordination of ICU procedures, were responsible for the positive medical outcome.
Permission from the patient and his family has been sought by CAM to publish these details on its website and elsewhere in the interests of accuracy. This permission was willingly provided and CAM expresses its thanks, admiration and respect.
CAM welcomes opportunities to provide similar professional support for registered medical practitioners and their patients.
http://www.camltd.co.nz/NZFPVol35No5Oct2008_Vitamin_C.pdf
http://drculik.blogspot.com/2008/07/lypospheric-vitamin-c.html
Books:Steve Hickey Book The Science of Vitamin C
Financial Disclosure: The author has no financial ties to disclose, nor financial ties to any vitamin C manufacturer or products mentioned in this article.
Jeffrey Dach MD
7450 Griffin Road Suite 190
Davie, Florida 33314
954-792-4663
http://www.drdach.com/
http://www.naturalmedicine101.com/
http://www.truemedmd.com/
http://www.bioidenticalhormones101.com/
Disclaimer click here: www.drdach.com/wst_page20.html
The reader is advised to discuss the comments on these pages with his/her personal physicians and to only act upon the advice of his/her personal physician. Also note that concerning an answer which appears as an electronically posted question, I am NOT creating a physician — patient relationship. Although identities will remain confidential as much as possible, as I can not control the media, I can not take responsibility for any breaches of confidentiality that may occur.
Link to this article: http://wp.me/P3gFbV-zD
Copyright (c) 2010-2013 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet without permission, provided there is a link to this page and proper credit is given. FAIR USE NOTICE: This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes.
Serving Areas of: Hollywood, Aventura, Miami, Fort Lauderdale, Pembroke Pines, Miramar, Davie, Coral Springs, Cooper City, Sunshine Ranches, Hallandale, Surfside, Miami Beach, Sunny Isles, Normandy Isles, Coral Gables, Hialeah, Golden Beach ,Kendall,sunrise, coral springs, parkland,pompano, boca raton, palm beach, weston, dania beach, tamarac, oakland park, boynton beach, delray,lake worth,wellington,plantation








Vitamin C Saves Man Dying of Viral Pneumonia - Jeffrey Dach MD July 21, 2013 at 8:28 AM
[…] Vitamin C Saves Dying Man […]
Vitamin C Saves Dying Man - Jeffrey Dach MD | L... August 9, 2013 at 4:06 AM
[…] Intravenous Vitamin C saves life of Allan Smith a New Zealand farmer dying of viral pneumonia.. […]
My Vitamins Are Killing Me Part Two - Jeffrey Dach MD July 20, 2014 at 7:21 AM
[…] Vitamin C Saves Dying Man In ICU […]
Geoffrey Leigh October 13, 2014 at 1:33 AM
Good on you Doctor. May 2013 i began manufacture of Liposomed Sodium Ascorbate and Liposomed Curcumin, within eight months i had four prostate tumor cases, on breast cancer and several schizophrenics symptom free and tumor markers 0.2 to nil.
How Does Cannabis Kill Cancer Cells Part Two - Jeffrey Dach MD October 26, 2014 at 1:04 PM
[…] Intravenous Vitamin C and other anti-oxidants are given to critically ill patients in the Intensive Care Unit. Vitamin C is a natural substance, a vitamin, so there are no drug company randomized trials. (Vitamin C Saves Life of Dying Man) […]
Dying man cured with vitamin C, doctors deny it. | occupy illuminati November 30, 2014 at 12:37 PM
[…] for “trying to sell supplements and alternative therapies” through his website. The Jefrey Dach M.D. […]
Vitamina C December 1, 2014 at 10:28 AM
[…] Vitamin C Saves Dying Man – Jeffrey Dach MD Mii de fructe si legume contin vitamina C. E o substanta inutila? Se stie ca fara vitamina C facem scorbut. Dar, se pare ca medicina vestica face tot ce poate ca sa uite treburile astea. Reply With Quote Homepage […]
Non-natural but alternative cancer cures | Pearltrees December 6, 2014 at 9:05 PM
[…] Vitamin C Saves Dying Man – Jeffrey Dach MD. By Jeffrey Dach MD The Allan Smith Story – TV Documentary Allan Smith, a New Zealand Dairy farmer, contracted Swine Flu while away on vacation in Fiji. […]
Natural Cancer Cures | Pearltrees December 6, 2014 at 9:07 PM
[…] Vitamin C Saves Dying Man – Jeffrey Dach MD. By Jeffrey Dach MD The Allan Smith Story – TV Documentary Allan Smith, a New Zealand Dairy farmer, contracted Swine Flu while away on vacation in Fiji. […]